Factors Associated with Clinical Adaptation among Newly Graduated Nurses: The Roles of Reality Shock and Resilience
Article information

Abstract
Background
This study was conducted to identify factors associated with clinical adaptation among newly graduated nurses, with particular focus on reality shock and resilience.
Methods
A cross-sectional study was conducted on 191 newly graduated nurses working at general hospitals in the Incheon area. Data were collected through an online survey. The collected data were analyzed using descriptive statistics, t-tests, correlation analysis, and multiple regression analyses.
Results
The mean clinical adaptation score was 5.77±1.80 on a 0–10 Visual Analogue Scale. Clinical adaptation was positively correlated with job satisfaction and resilience and negatively correlated with reality shock. Job satisfaction (β=0.17, P=0.017), adaptability (β=0.24, P=0.008), and lack of confidence (β=–0.43, P<0.001) were significantly associated with clinical adaptation, accounting for 45.9% of the variance (adjusted R2=0.459).
Conclusions
Interventions aimed at enhancing resilience, strengthening confidence in clinical practice, and promoting positive work experiences may facilitate successful clinical adaptation among newly graduated nurses. These findings provide evidence for the development of targeted support strategies to promote a successful transition to professional nursing practice.
INTRODUCTION
One of the key factors determining the quality of medical services and a hospital’s competitiveness is the retention of skilled nursing staff [1]. However, the high turnover rate among newly graduated nurses has been identified as a significant challenge in human resource management for healthcare institutions.
According to data from the Hospital Nurses Association [2], 47.7% of the 23,064 newly graduated nurses hired in 2020 resigned within 3 years, and among them, 3,599 nurses (15.6%) resigned within 1 year of hire. The primary reason for resignation was inability to adapt to the job (36.5%). This findings suggest that the clinical adaptation among newly graduated nurses is a critical challenge in nursing workforce management [3,4].
Newly graduated nurses face complex demands including role burden, time pressure, responsibility for patient safety, and interpersonal relationships, as they provide patient care while collaborating with various healthcare staff in a new hospital environment [4-6]. In particular, they experience reality shock [5,7], defined as a psychological conflict characterized by feelings of helplessness and emptiness arising from the discrepancy between the professional role expected during nursing education and the realities of clinical practice. This phenomenon is a major stressor associated with the clinical adaptation of newly graduated nurses [6].
Individual psychological resources have also been identified as important factors in the clinical adaptation of newly graduated nurses [8]. Resilience refers to an individual’s psychological capacity to maintain psychological balance, adapt positively, and achieve growth in the face of stressful situations or difficult environments [9]. Individuals with high resilience are more likely to cope more effectively with various difficulties experienced in the work environment and demonstrate positive outcomes in the process of organizational adaptation [10,11].
However, the adaptation of newly graduated nurses should be understood as a multidimensional process that results from continuous interactions between individuals and their environments. To provide a theoretical explanation for this process, the present study was guided by Roy’s Adaptation Model (RAM) [12]. According to RAM, individuals are adaptive systems that continuously respond to environmental stimuli through coping processes, resulting in adaptive or ineffective responses [12,13]. Environmental stimuli may challenge an individual’s adaptive capacity, whereas coping mechanisms facilitate adjustment and adaptation. Within this framework, reality shock can be conceptualized as an environmental stimulus arising from discrepancies between educational expectations and clinical realities [7,14], while resilience represents an internal coping mechanism that enables individuals to respond effectively to such challenges [9,15]. Clinical adaptation, therefore, can be viewed as an adaptive response resulting from the interaction between reality shock and resilience. Applying RAM provides a useful framework for understanding how newly graduated nurses adjust to professional practice and for identifying factors that promote successful adaptation.
Therefore, this study aimed to identify factors associated with clinical adaptation among newly graduated nurses, focusing on reality shock and resilience. The findings of this study may provide useful evidence for developing interventions and nursing management strategies to support the clinical adaptation of newly graduated nurses.
METHODS
Design
This cross-sectional study was conducted to identify factors associated with clinical adaptation among newly graduated nurses, with a particular focus on reality shock and resilience.
Participants
The study participants were newly graduated nurses with less than 1 year of clinical experience working in general hospitals. Participants were recruited through convenience sampling from newly graduated nurses employed at general hospitals in the Incheon region. The required sample size was calculated using the G*Power 3.1.9.7 program for multiple linear regression analysis. Assuming an effect size of 0.15 [16], a significance level of 0.05, and a statistical power of 0.80, the minimum sample size was determined to be 169. Considering a potential dropout rate of 15%, the online survey was designed to collect a total of 200 responses. After excluding nine incomplete questionnaires, data from 191 participants were included in the final statistical analysis.
Measurement
In this study, a structured questionnaire was used to assess general characteristics, job-related characteristics, reality shock, resilience, and clinical adaptation.
General and job-related characteristics
To identify the participants’ general and job-related characteristics, the following variables were collected: sex, age, living arrangement, prior experience working at other hospitals, working department, duration of clinical experience, placement in the desired department, experience with preceptor training, and job satisfaction. Job satisfaction was assessed on a 5-point Likert scale and subsequently categorized into two groups: not satisfied (1–3 points) and satisfied (4–5 points).
Reality shock
Reality shock was measured using the Reality Shock Measurement Tool for Newly Graduated Nurses developed by Yun [17]. This tool consists of 26 items and includes five subdomains: disappointment to reality, overwhelming task, lack of confidence, heavy responsibility, and lack of support. Each item is measured on a 5-point Likert scale ranging from 1 (“not at all”) to 5 (“very much so”), with higher scores indicating greater levels of reality shock. In Yun’s [17] study, Cronbach’s α was 0.93, with subscale reliabilities ranging from 0.73 to 0.89. In this study, Cronbach’s α was 0.94, and the subscale reliabilities ranged from 0.93 to 0.94.
Resilience
Resilience was measured using the Korean version of the Connor-Davidson Resilience Scale (K-CD-RISC) [9], translated by Lee [18] from the original scale developed by Connor and Davidson [9]. This tool consists of 25 items and comprises seven subdomains: hardiness, optimism, coping, adaptability, meaningfulness/purpose, regulation of emotion and cognition , and self-efficacy. Each item is measured on a 5-point Likert scale ranging from 0 (“not at all”) to 4 (“very much so”) with higher scores indicating greater resilience. In the study by Connor and Davidson [9], Cronbach’s α was 0.89, whereas in this study, it was 0.93.
Clinical adaptation
Adaptation is defined as a dynamic process and outcome resulting from the interaction between individuals and their environment [12]. In this study, the level of clinical adaptation among newly graduated nurses was measured using a single-item Visual Analogue Scale (VAS) from 0 to 10. Single-item measures, such as the VAS, may be appropriate for assessing global and holistic constructs that individuals can clearly recognize and evaluate. Previous studies have demonstrated that this approach has acceptable reliability and validity for measuring constructs such as adaptation [13,19,20]. Unlike adaptability, which reflects an individual’s coping capacity, clinical adaptation in this study refers to the perceived outcome of adjustment to the clinical environment.
Ethical considerations
This study was conducted after obtaining approval (No. 1044396-202209-HR-178-01) from the Institutional Review Board of Gachon University prior to data collection. The study was conducted in accordance with the ethical principles set forth in the Declaration of Helsinki. The instruments used in this study were applied with permission from the original authors. Data collection was carried out after explaining the purpose and methods of the study to the nursing departments of the participating hospitals and obtaining their cooperation. Participants voluntarily completed the survey after providing informed consent, having been informed online about the purpose and procedures of the study, assurance of anonymity, and the right to withdraw at any time. Participants who completed the online survey were provided with a small incentive. The collected data were coded and analyzed anonymously and were used solely for the purposes of this study.
Data collection procedure
To collect data, the purpose and methods of the study were explained to the nursing departments of five general hospitals in the Incheon region, and their cooperation was obtained. Data collection was conducted over a 4-week period from October 21 to November 16, 2022. Recruitment of study participants was conducted through internal hospital announcements, and a guide containing the purpose and procedures of the study was posted online. Newly graduated nurses voluntarily accessed the online survey link, reviewed the informed consent form, and completed the survey upon providing consent. The survey was configured so that the link would be automatically closed once the target sample size was reached.
Statistical analysis
Data analysis was performed using IBM SPSS Statistics version 26.0 (IBM Corp.). The general and job characteristics of the study participants were analyzed using descriptive statistics, including frequencies, percentages, means, and standard deviations. Reality shock, resilience, and clinical adaptation were analyzed using descriptive statistics, such as means and standard deviations. Differences between groups were analyzed using t-tests, ANOVA, and chi-square tests, while post hoc testing was performed using the Scheffé test. The relationships between reality shock, resilience, and clinical adaptation were analyzed using Pearson’s correlation coefficients. Prior to the multiple regression analysis, the assumptions of normality, homoscedasticity, independence of residuals, and multicollinearity were examined. Multicollinearity was assessed using tolerance and variance inflation factor (VIF) values. Multiple regression analysis was conducted to identify factors associated with clinical adaptation among newly graduated nurses, with the statistical significance level set at P<0.05.
RESULT
General and job-related characteristics of participants
The general and job-related characteristics of the participants are presented in Table 1. Approximately 82% of the participants were female, and the mean age was 24.27±2.22 years. Regarding living arrangements, living alone was the most common (44.5%), followed by living with family (38.2%) and living with friends or colleagues (17.3%). Approximately 88.5% of participants had no prior work experience at other hospitals. In terms of working department, surgical wards were the most common (33.0%), followed by internal medicine (27.7%), other specialized departments (22.5%), and intensive care units (16.8%). The mean duration of clinical experience was 6.08±2.63 months. A total of 90.1% of participants received preceptor training, and among them. The average level of job satisfaction was 3.31±0.75 out of 5 points.
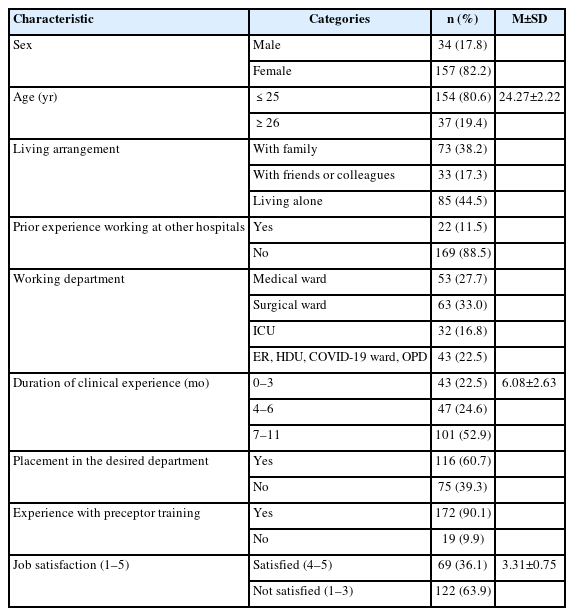
Demographic and job-related characteristics of participants (N=191)
Regarding clinical adaptation, 78.0% of participants were classified as adapted, while 22.0% were classified as non-adapted.
Reality shock, resilience, and clinical adaptation
The mean score for reality shock among participants was 2.98±0.66. By subdomain, ‘lack of confidence (3.27±0.80)’ and ‘overwhelming task (3.22±0.87)’ were relatively high, whereas ‘lack of support (2.17±0.74)’ was the lowest. The mean resilience score was 2.35±0.53. Among the subdomains, ‘coping (2.56±0.57)’ and ‘self-efficacy (2.52±0.76)’ were high, whereas ‘regulation of emotion and cognition (2.01±0.80)’ was low. The mean clinical adaptation score measured was 5.77±1.80 (Table 2). Clinical adaptation levels differed significantly according to duration of clinical experience (P=0.012) and nursing job satisfaction (P=0.001) (Table 3).
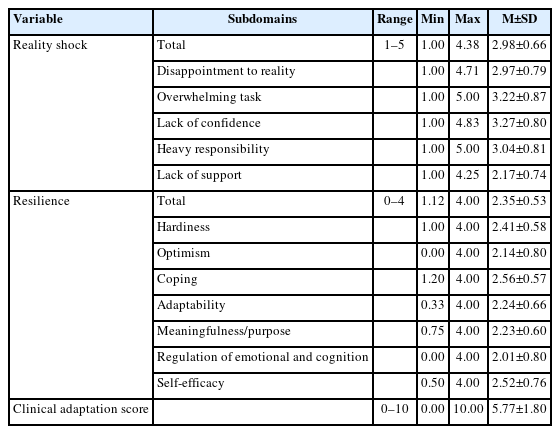
Descriptive statistics of reality shock, resilience, and adaptation (N=191)
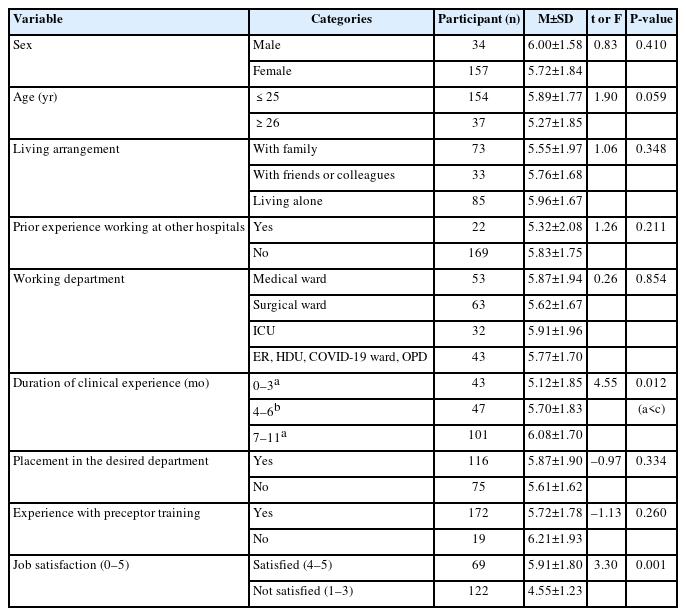
Differences in clinical adaptation status according to participant characteristics (N=191)
Clinical adaptation was positively correlated with job satisfaction (r=0.43, P<0.01) and all subdomains of resilience, including hardiness (r=0.43, P<0.01), optimism (r=0.32, P<0.01), coping (r=0.45, P<0.01), adaptability (r=0.55, P<0.01), meaningfulness/purpose (r=0.39, P<0.01), regulation of emotion and cognition (r=0.40, P<0.01), and self-efficacy (r=0.45, P<0.01). In contrast, clinical adaptation was negatively correlated with the reality shock subdomains of lack of confidence (r=–0.62, P<0.01), heavy responsibility (r=–0.43, P<0.01), lack of support (r=–0.37, P<0.01), and overwhelming (r=–0.42, P<0.01). Among these variables, lack of confidence showed the strongest negative correlation, whereas adaptability demonstrated the strongest positive correlation with clinical adaptation (Table 4).
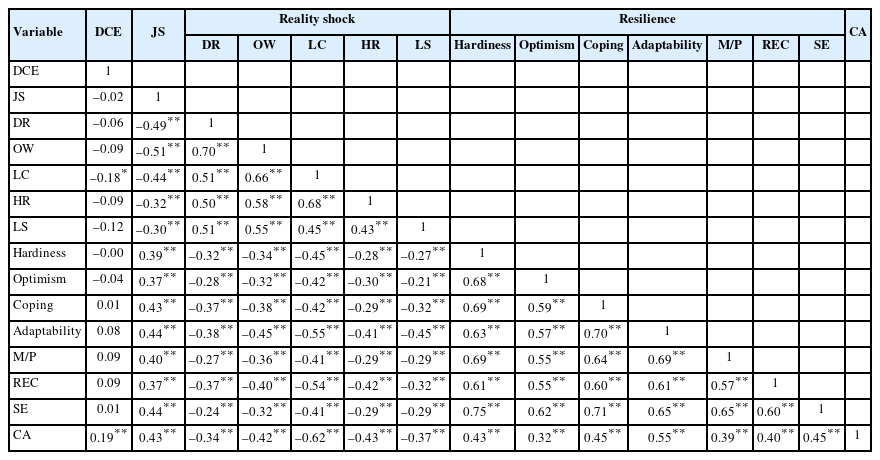
Correlations among the major study variables (N=191)
Factors associated with clinical adaptation
Duration of clinical experience and job satisfaction, which showed significant differences in clinical adaptation in the univariate analyses, were included as covariates in the multiple regression model along with the subdomains of reality shock and resilience. Prior to conducting the multiple linear regression analysis, the assumptions of normality, homoscedasticity, independence of residuals, and multicollinearity were examined. Residual normality was assessed using histograms and normal probability plots, and homoscedasticity was evaluated through standardized residual scatterplots. Multicollinearity was assessed using tolerance and variance VIF values. Tolerance values ranged from 0.299 to 0.924 and VIF values ranged from 1.083 to 3.346, indicating no evidence of problematic multicollinearity.
Multiple linear regression analysis revealed that job satisfaction (β=0.17, P=0.017), adaptability, a subdomain of resilience (β=0.24, P=0.008), and lack of confidence, a subdomain of reality shock (β=–0.43, P<0.001), were significant factors associated with clinical adaptation. Specifically, higher levels of job satisfaction and adaptability were associated with better clinical adaptation, whereas greater lack of confidence was associated with poorer clinical adaptation. The regression model explained 45.9% of the variance in clinical adaptation (adjusted R2=0.459) and was statistically significant (F=12.50, P<0.001) (Table 5).
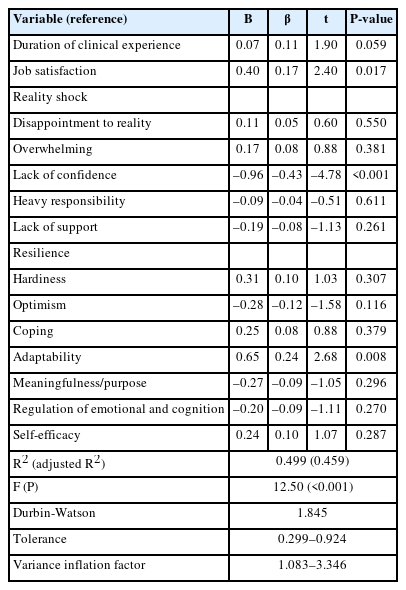
Multiple linear regression analysis of factors associated with clinical adaptation (N=191)
DISCUSSION
Implication for nursing management
This study was conducted to identify factors associated with clinical adaptation among newly graduated nurses, focusing on reality shock and resilience. The findings of this study showed that adaptability, a sub-domain of resilience, and job satisfaction had a significant positive association with the clinical adaptation, while lack of confidence, sub-domains of reality shock, showed a significant negative association with clinical adaptation of newly graduated nurses. These findings are consistent with previous studies showing that resilience positively related to the organizational socialization and adaptation of newly graduated nurses. Recent studies have demonstrated that resilience is a significant factor enhancing organizational socialization and job performance among new nurses, thereby facilitating their adaptation to clinical settings [17,21]. Furthermore, resilience has been identified as an important personal resource that supports nurses’ psychological functioning and adaptation in stressful work environments [15]. It is also associated with improved clinical competence and retention-related outcomes in newly graduated nurses [11,12,22].
In particular, the fact that adaptability was found to be a significant factor associated with clinical adaptation among the sub-domains of resilience suggests that it plays a key role in achieving functional adaptation by flexibly regulating one’s emotions and behaviors amidst the various stresses and environmental changes experienced by newly graduated nurses in the clinical setting [20]. Rather than simply coping, adaptability appears to support more flexible regulation of emotions and behaviors, as well as the ongoing adjustment of coping strategies to fit situational demands. Therefore, to improve the clinical adaptation of newly graduated nurses, it is necessary to develop educational programs that can strengthen resilience, along with establishment of a systematic coaching and mentoring system [23].
The results of this study, which identified lack of confidence as a major factor related to clinical adaptation among the sub-domains of reality shock, suggest that individual psychological resource play important role in the clinical adaptation process of newly graduated nurses. This finding is consistent with previous studies indicating that the reality shock experienced by newly graduated nurses stems from the gap between nursing education and actual clinical practice [7], and that this gap acts as a factor hindering adaptation [5,6,21]. In particular, these findings are closely linked to the concept of ‘transition shock’ experienced by newly graduated nurses upon entering the clinical field [14]. Transition shock is a complex stress arising from role changes, increased responsibilities, and the gap between expectations and reality, which can has been associated with difficulties in initial adaptation and turnover [14]. In this context, lack of confidence can be understood as a factor that intensify this transition process. Furthermore, a lack of confidence signifies psychological vulnerability associated with a lack of self-efficacy regarding clinical performance, which can be related to be delayed clinical adaptation by inducing passive responses in decision-making and problem-solving processes in new environments.
In addition, support provided by preceptors and fellow nurses is reported to be a key factor in promoting job adaptation by facilitating the emotional stability and learning of new nurses and reinforcing confidence in performing their roles within the organization [8,24,25]. Therefore, to reduce the reality shock of newly graduated nurses and support their successful clinical adaptation, it is essential to implement education and feedback-based interventions that can strengthen individual confidence.
Although the association between clinical experience and clinical adaptation did not reach statistical significance, the direction of the relationship suggested that nurses with longer clinical experience tended to report higher levels of clinical adaptation. This pattern is in line with previous research indicating that adaptation experiences during the early employment period may influence later organizational adaptation and turnover [3,4]. The tendency observed in this study may be attributable to the accumulation of clinical experience, which can facilitate professional competence, role clarity, and confidence in navigating the clinical environment. Therefore, continued efforts to provide structured educational support and ongoing adaptation assistance for newly graduated nurses may be beneficial. The present study also identified nursing job satisfaction as a significant factor associated with clinical adaptation.
The present study identified nursing job satisfaction as a significant factor associated with clinical adaptation among newly graduated nurses. Nurses who reported higher levels of job satisfaction demonstrated better adaptation to the clinical environment. This finding is consistent with previous studies suggesting that positive work experiences facilitate organizational socialization, professional growth, and successful role transition among newly graduated nurses [4,14,23]. Job satisfaction may enhance motivation, professional commitment, and engagement in learning and clinical practice, thereby promoting adaptation to the demands of the clinical setting. Conversely, dissatisfaction may increase stress and be associated with difficulties in adjustment during the transition from student to professional nurse. Given that successful adaptation is closely linked to organizational socialization processes [25,26], healthcare organizations should not only provide clinical competency training but also foster supportive work environments that promote job satisfaction among newly graduated nurses.
Meanwhile, although this study measured and analyzed adaptation as a single concept, according to RAM, adaptation is understood as a multidimensional process achieved through the interaction between the individual and the environment [12]. In particular, the four modes of adaptation—physiological, self-concept, role-function, and interdependence—provide a framework that can more comprehensively explain nurses’ clinical adaptation. From this perspective, lack of confidence may reflect challenges in the self-concept mode, whereas greater clinical experience may contribute to role-function stabilization. Adaptability may support balance across multiple adaptive modes by facilitating effective responses to changing clinical demands. Furthermore, these findings support Roy’s proposition that adaptation is influenced by the interaction between stimuli and coping mechanisms. In the present study, lack of confidence may function as a stimulus that challenges adaptation, while adaptability may represent an individual’s coping capacity that enables effective responses to such challenges, which may be associated with successful clinical adaptation.
It is important to note that lack of confidence, adaptability, and clinical adaptation represent conceptually distinct constructs within Roy’s adaptation process. Lack of confidence reflects a psychological perception of environmental demands and may function as a contextual stimulus, whereas adaptability represents an internal coping capacity that facilitates flexible responses to changing situations. In contrast, clinical adaptation reflects the outcome of these adaptive processes and indicates the extent to which newly graduated nurses have successfully adjusted to and integrated into the clinical work environment [12,13].
In summary, the clinical adaptation of newly graduated nurses can be understood as a complex process involving the interaction of personal and organizational environmental factors, which can be explained as a process of organizational socialization in which individuals learn and internalize the norms and roles of the organization [26]. Overall, these findings underscore the need to address both individual and organizational factors in an integrated manner. Therefore, to improve the clinical adaptation of newly graduated nurses, a multi-layered approach is required that establishes systematic socialization strategies and a supportive environment at the organizational level, along with interventions that strengthen individual competencies and psychological resources.
Limitation and future directions
This study has several limitations. First, because the study was conducted among newly graduated nurses working in general hospitals located in specific regions, caution is needed when generalizing the findings to all newly graduated nurses. Second, data were collected through self-reported online questionnaires, which may have introduced social desirability bias and limited the extent to which responses reflected actual experiences. Third, the cross-sectional design precludes the establishment of causal relationships among the study variables. In addition, clinical adaptation was measured using a single-item VAS. Although previous studies have supported the usefulness and practicality of single-item measures for assessing overall perceptions and attitudes [20], such measures may not fully capture the multidimensional nature of clinical adaptation. Clinical adaptation encompasses various domains, including professional competence, role adjustment, interpersonal relationships, and organizational integration. Future research should therefore employ standardized multidimensional instruments that can more comprehensively assess the complexity of clinical adaptation among newly graduated nurses. Furthermore, future studies should include a broader range of hospital settings and geographic regions to better reflect diverse clinical environments. Longitudinal research is also needed to examine changes in clinical adaptation over time and to clarify the causal relationships among factors influencing adaptation.
Conclusions
This cross-sectional study examined the relationships of reality shock and resilience with clinical adaptation among newly graduated nurses and identified factors associated with adaptation. The results showed that reality shock was negatively associated with clinical adaptation, whereas resilience was positively associated. In particular, adaptability, a subfactor of resilience, and job satisfaction were positively associated with adaptation, while lack of confidence, a subfactor of reality shock, was negatively associated with adaptation. These findings suggest that successful clinical adaptation among newly graduated nurses is related to both individual psychological resources and work-related experiences. In particular, adaptability appears to facilitate adaptation during the transition to professional practice, whereas lack of confidence may hinder this process. Therefore, efforts to enhance resilience, strengthen confidence in clinical practice, and promote job satisfaction may contribute to improving clinical adaptation among newly graduated nurses. Therefore, organizational efforts to enhance job satisfaction and support resilience development may help facilitate successful clinical adaptation among newly graduated nurses.
Notes
AUTHOR CONTRIBUTIONS
Dr. Young KO had full access to all of the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis. All authors (reviewed this manuscript and agreed to individual contributions.
Conceptualization: all authors. Data collection SHK. Formal analysis: all authors. Investigation: SHK. Methodology: all authors. Writing–original draft: SHK. Writing–review & editing: YK.
CONFLICTS OF INTEREST
Young KO is the Associate Editor of this journal and was not involved in the peer review or editorial decision-making process for this article. No other potential conflicts of interest relevant to this article were reported.
FUNDING
None.
DATA AVAILABILITY
The datasets presented in this study are available upon reasonable request from the corresponding author.
ACKNOWLEDGMENTS
This article is based on a part of the first author's master’s thesis (or doctoral dissertation) from Gachon University.