How People Decide to Protect Their Health: A Protection Motivation Theory–Theory of Reasoned Action Perspective
Article information

Abstract
Background
This study investigated how perceived knowledge, threat, and coping appraisals, moral obligation, and social approval influence voluntary mask-wearing intentions within an integrated framework combining Protection Motivation Theory (PMT) and the Theory of Reasoned Action (TRA). Understanding the drivers of protective behaviors after mandates are lifted is essential for sustaining public health practices. In the United States—where mask wearing is not culturally normative—such behaviors rely on internal motivations rather than external enforcement.
Methods
Using data from a nationwide online survey of 360 U.S. adults, structural equation modeling was employed to test relationships among perceived knowledge, threat appraisal, coping appraisal, moral obligation, social approval, and behavioral intention.
Results
Perceived knowledge significantly predicted both coping and threat appraisals. Coping appraisal influenced moral obligation, while threat appraisal affected both moral obligation and social approval. Among all predictors, only moral obligation significantly predicted behavioral intention, which in turn predicted protective behavior.
Conclusions
These findings highlight the central role of moral obligation and coping appraisal as key drivers of voluntary health protective intentions. The integrated PMT–TRA model provides actionable insights for sustaining motivation in low-threat contexts and offers guidance for shaping future public health strategies.
INTRODUCTION
Seasonal influenza activity has increased globally since October 2025, with influenza A (H3N2) predominant and co‑circulation of other respiratory viruses such as respiratory syncytial virus (RSV) [1]. In the U.S., influenza infections are growing or are likely to grow in 47 states, RSV is rising in multiple regions, and COVID-19 activity is trending upward [2]. These concurrent viral trends demonstrate that respiratory infectious diseases continue to pose substantial public health risks even after the acute phase of the COVID-19 pandemic. The COVID-19 pandemic itself profoundly reshaped global health behaviors, resulting in millions of infections and deaths worldwide by late 2024 [3,4]. Before vaccines became widely available in early 2021, non‑pharmaceutical interventions (NPIs), including social distancing, quarantine, and mask use, were essential for reducing viral transmission [5,6]. Public health authorities consistently promoted mask‑wearing, hand hygiene, and physical distancing as primary preventive strategies [7-9], reflecting longstanding evidence that these behaviors mitigate respiratory infection risks in shared environments [7]. Scientific support for mask effectiveness, reinforced by clear public health messaging, contributed to widespread acceptance of mask use during the pandemic [7,10,11]. As societies transition away from mandated NPIs, understanding the psychological and social drivers of voluntary protective practices becomes increasingly important for future preparedness. Although mask‑wearing initially emerged as a mandated public health measure, its continuation in voluntary contexts reflects complex psychological, social, and expressive dimensions. Studies indicate that masks do not necessarily impede social interaction [12] and can even enhance aspects of self‑expression [13]. These findings suggest that mask use carries multifaceted meanings (e.g., protective, social, and symbolic), highlighting the need for theoretical perspectives that extend beyond compliance‑based explanations [14-16].
To address this gap, this study integrated Protection Motivation Theory (PMT) and the Theory of Reasoned Action (TRA) [14-17]. PMT explains health‑protective behavior through threat appraisal (perceived severity and vulnerability) and coping appraisal (self‑efficacy, response efficacy, and perceived costs) [18-20]. TRA emphasizes the role of attitudes and subjective norms in shaping behavioral intention, including moral obligation as an internalized motivation to behave responsibly toward others [14,21]. Although extensive research has examined protective behaviors during mandatory enforcement periods, few studies have integrated PMT and TRA to investigate voluntary mask-wearing in post-mandate, low-risk settings. To address this gap, this study applies an integrated PMT–TRA framework to examine the psychological and social determinants of voluntary health-protective behavior. Therefore, this study aimed to investigate how perceived knowledge, threat appraisal, coping appraisal, social approval, and moral obligation collectively shape individuals’ intentions and mask‑wearing behavior within an integrated PMT–TRA framework. By identifying these determinants, the study extends theoretical understanding of voluntary health‑protective behaviors in the post‑mandate era and offers actionable insights for public health communication and preparedness strategies.
Protection motivation theory
PMT explains how people evaluate a health threat and their ability to cope with it when deciding whether to engage in protective behaviors [16,17]. Two interrelated processes (threat appraisal and coping appraisal) jointly shape protection motivation. Threat appraisal reflects the perceived severity, vulnerability, and the rewards of not acting; higher perceived severity and vulnerability, along with lower maladaptive rewards, support adaptive action [22,23]. Coping appraisal reflects beliefs about response efficacy, self-efficacy, and response cost; stronger efficacy beliefs and lower perceived costs promote protective behavior [20,23].
PMT has been widely applied to health and environmental actions. For example, hope and fear dynamics predicted adaptive changes during the pandemic [22], and classic experiments demonstrated how PMT components drive adaptive versus maladaptive coping [23]. Beyond infectious disease, PMT has explained sustainable behaviors such as waste management [24] and offers practical guidance for persuasive health communication [25]. Empirical COVID-19 research also links threat and coping processes to adherence behaviors (e.g., social distancing) across countries [26] and to vaccination intentions in diverse contexts [27,28]. Because appraisal processes depend on what people know, perceived knowledge is a precursor to both coping and threat appraisals, and often predicts stronger intentions to act [27,28]. Furthermore, threat and coping appraisals are central drivers of adaptive protective behavior [21,29,30]. Stronger coping appraisal (higher self-/response efficacy, lower cost) encourages adherence to guidelines and reduces maladaptive responses [31]. Based on the view that appraisals can activate social (normative) and moral (attitudinal) motives, we proposed:
H1. Perceived knowledge positively affects (a) coping appraisal and (b) threat appraisal.
H2. Coping appraisal positively affects (a) social approval and (b) moral obligation.
H3. Threat appraisal positively affects (a) social approval and (b) moral obligation.
Theory of reasoned action (adaptive responses)
The TRA posits that behavioral intention, the most immediate predictor of behavior, arises from attitude toward the act and subjective norm (perceived social pressure) [32]. In health contexts, subjective norms reflect expectations from family, friends, and peers. Observing peers who reject masking weakens compliance, whereas supportive norms reinforce it [33-35]. In this study, attitude is conceptualized as moral obligation—an internalized sense of duty to protect others. Moral obligation sustains prosocial action when external enforcement is low and has been shown to predict collective preventive behaviors during health crises [36-38]. Finally, extensive meta-analytic evidence confirmed that behavioral intention consistently predicts actual behavior across diverse health domains [39].
H4. Social approval (subjective norm) positively influences behavioral intention.
H5. Moral obligation (attitude) has a positive effect on behavioral intention.
H6. Behavioral intention positively affects behavior.
Integrated framework for health-protective behavior
Drawing on the literature reviewed above, this study integrated PMT and TRA into a unified conceptual framework to explain voluntary health-protective behavior. PMT accounts for how individuals appraise health threats and their capacity to respond effectively, while TRA addresses the role of social norms and attitudinal factors in forming behavioral intentions. This integrated framework provides a more comprehensive account of protective behaviors, such as mask-wearing, in post-mandate contexts, where continued engagement depends on internal motivation rather than an external mandate (Fig. 1).
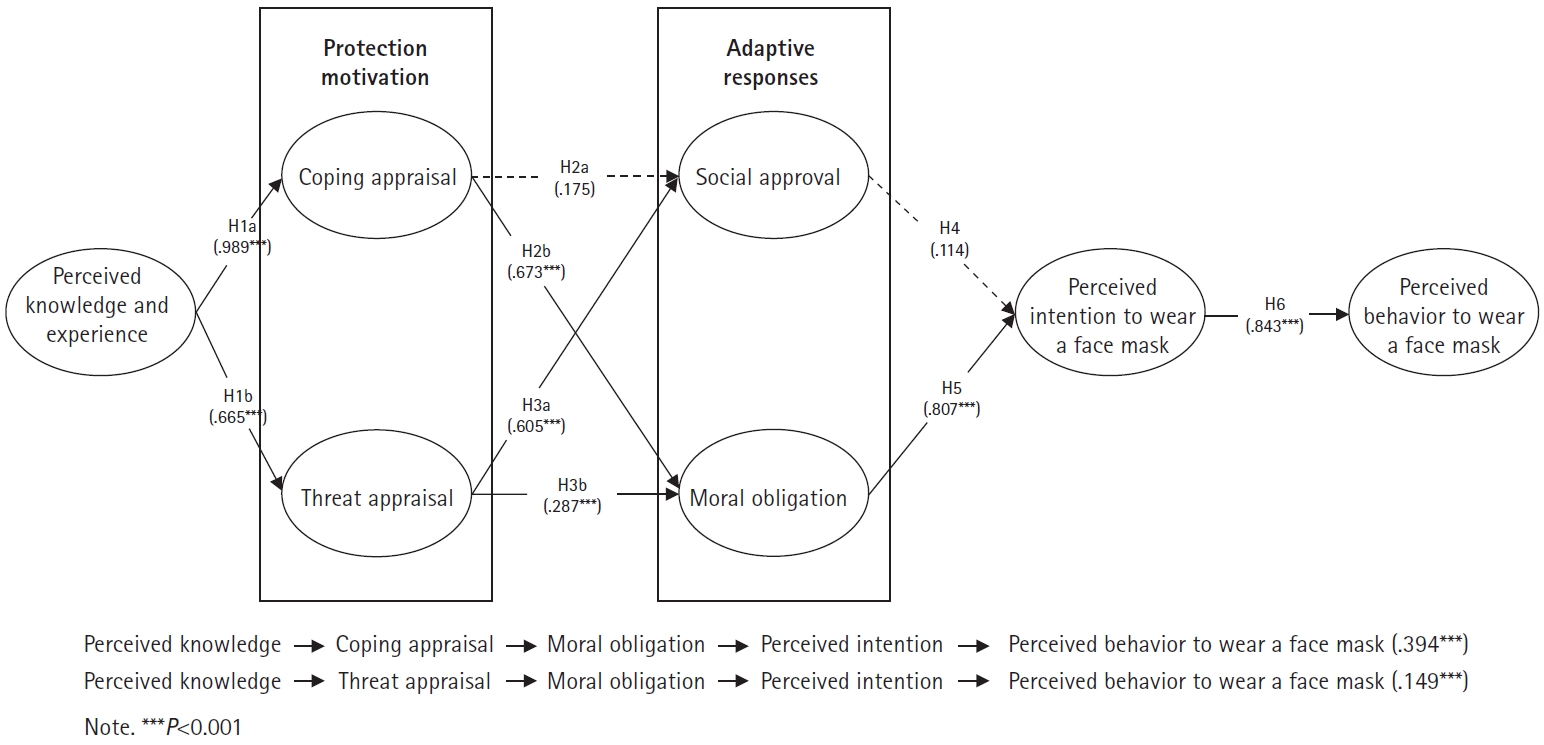
Hypothesis testing for indirect and direct paths.
METHODS
Sample and sampling
A web-based survey questionnaire was employed for this study. The online survey collected a nationwide convenience sample of consumers in the United States through a crowdsourcing marketplace (e.g., MTurk). The study was approved by the Institutional Review Board (IRB) of Florida State University (IRB No. STUDY# 00002266). This study used a face mask as a stimulus to examine health-protective behavior. Using a face mask in this type of research is considered appropriate because it is a visible and widely recognized health-protective behavior during infectious disease outbreaks. It effectively represents individuals’ perceptions of risk, susceptibility, and motivation to protect their health. Additionally, the use of a mask highlights how attitudes, perceived knowledge, and social norms influence health-protective practices.
The online survey took approximately 19 minutes to complete. A total of 587 surveys were initially completed by individuals in the United States who wore face masks during the COVID-19 pandemic. The final sample was reduced from 587 to 404 surveys due to the deletion of cases with incomplete questionnaires. In addition, qualification questions (e.g., frequency, types of masks) were included to filter out inattentive and bot responses. For example, respondents were first asked to provide answers about their mask usage behavior. Then, the survey presented images of different types of masks (i.e., surgical, fashion, N95, natural fabric). Incorrect responses were removed. In addition, responses completed in a relatively short time (10 minutes) and straightliners (identical values across all items) were excluded to ensure data quality. Finally, the data were examined to detect multivariate outliers using z-score screening [40]. Raw scores were transformed into z-scores, and values that exceeded |2.58| were removed. After applying these screening procedures, 360 data were retained for further analysis.
Instrument
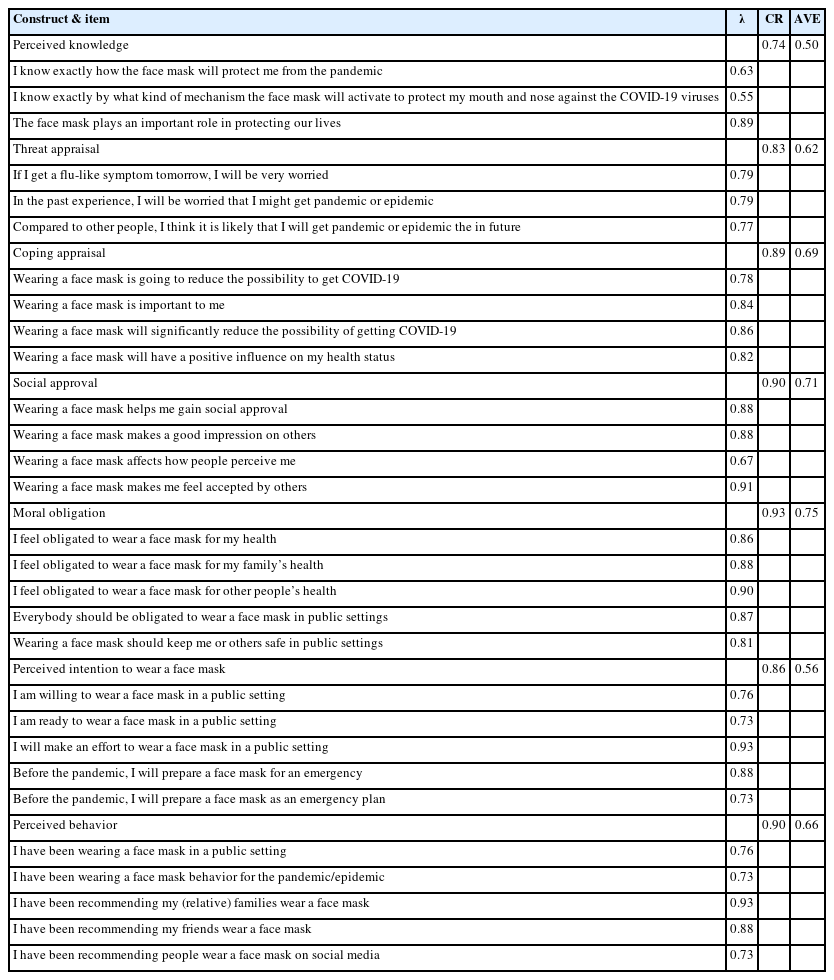
The survey questionnaire consisted of two sections: demographics and constructs with multiple-item measurements adapted and modified from previous research [41-44]. To test the hypothesized paths in the proposed conceptual framework, multiple-item measurements: perceived knowledge (three items), threat appraisal (three items), coping appraisal (four items), social approval (four items), moral obligation (five items), perceived intention (five items), and perceived behavior (five items), were anchored on a 7-point Likert-type scale.
Data analyses
SPSS 29 (IBM Corp.) and Mplus 9 statistical packages (Muthén & Muthén) were used to achieve this study’s purpose and test hypotheses. With SPSS 29, descriptive analysis was conducted to analyze preliminary results and determine sample demographics. Using Mplus 9, confirmatory factor analysis was performed to validate the psychometric properties of the measured variables, while structural equation modeling (SEM) was employed to test the hypotheses.
RESULTS
Demographic analysis
Of the 360 respondents, male participants were 48.3% (n=174) with an average age of 43.78, while 30.0% (n=108) had annual incomes between $50,000 and $74,999. The majority of the respondents were full-time employees and had a college degree (n=216). A total of 74.7% of respondents were Caucasian, followed by Asian (13.3%) and African American (6.1%).
Preliminary analysis
Mardia’s coefficients were used to construct multivariate skewness and kurtosis to test the multivariate normality assumption. Multivariate skewness (z=270.184, standard deviation [SD]=1.92, P<0.001) and multivariate kurtosis (z=1,442.32, SD=4.30, P<0.001) were found to be significant, indicating a violation of the multivariate normality assumption. To mitigate the non-normal distribution, we employed a robust estimation technique, specifically maximum likelihood mean-adjusted estimation, in our data analyses [45].
Measurement validation
The psychometric properties of the measurement model are reported in Table 1. The internal consistency of the latent variables was examined using Cronbach’s alpha. All Cronbach’s alpha coefficients for the variables were greater than 0.70. Additionally, composite reliability values exceeded 0.70. Factor loadings (λ) for each item within the measured latent variables were assessed to examine the strength of the relation between the latent variable and item (λ>0.50) [46]. One item in the coping appraisal was removed due to the low factor loading. The revised measurement was assessed, and factor loadings exceeded the suggested threshold of 0.50. The average variance extracted (AVE) was also assessed to understand whether the factor explains more variance than error [47]. All AVE values of the latent variables were greater than 0.50. Based on the results, the convergent validity was identified in this study.
The measurement model
Moreover, discriminant validity was tested using the Heterotrait-Monotrait ratio (HTMT) of the correlations [48]. According to Henseler et al. [49], an issue arises with discriminant validity when HTMT values exceed 0.85. In this study, discriminant validity was ensured because all HTMT values were lower than 0.85 (Table 2). Finally, the measurement model demonstrated an acceptable fit of the data (Satorra-Bentler scaled chi-square [S-B χ2] =792.73, degree or freedom [df]=351, S-B χ2/df=2.51, Comparative Fit Index [CFI]=0.933, Root Mean Square Error of Approximation [RMSEA]=0.06, Standardized Root Mean Square Residual [SRMR]=0.05).
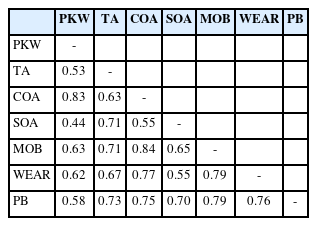
Assessment of discriminant validity using HTMT
Exploratory results
After confirming the psychometric properties of the measurement model, we proceeded with SEM to test the hypotheses in this study. The SEM demonstrated acceptable fit (S-B χ2=1,142.43, df=449, S-B χ2/df=2.54, CFI=0.909, RMSEA=0.06, SRMR=0.07). In terms of hypothesis testing, SEM revealed that perceived knowledge had a significant effect on coping appraisal (H1a: β=0.989, standard error [SE]=0.017, P<0.001) and threat appraisal (H1b: β=0.665, SE=0.052, P<0.001). Only coping appraisal had a significant effect on moral obligation (H2b: β=0.673, SE=0.064, P<0.001), but there was no significant effect on social approval (H2a: β=0.175, SE=0.120, P<0.110). Threat appraisal positively affected social approval (H3a: β=0.605, SE=0.010, P<0.001) and moral obligation (H3b: β=0.287, SE=0.070, P<0.001). Perceived intention to wear a face mask was only significantly associated with moral obligation (H5: β=0.807, SE=0.063, P<0.001), but not social approval (H4: β=0.114, SE=0.075, P=0.127). Lastly, the perceived intention to wear a face mask significantly influenced perceived behavior (H6: β=0.843, SE=0.046, P<0.001).
Additional post hoc analyses were conducted to investigate mediating effects. Perceived knowledge did not have significant positive effects on perceived behavior through coping appraisal, social approval, and perceived intention to wear a face mask (β=0.013, SE=0.016, P=0.417; 95% confidence interval [CI]=–0.016 to 0.075) and through threat appraisal, social approval, and perceived intention to wear a face mask (β=0.071, SE=0.051, P=0.165; 95% CI=–0.006 to 0.101). In contrast, perceived knowledge had significant positive effects on perceived behavior through coping appraisal, moral obligation, and perceived intention to wear a face mask (β=0.394, SE=0.062, P<0.001; 95% CI=0.274–0.514) and through threat appraisal, moral obligation, and perceived intention to wear a face mask (β=0.149, SE=0.036, P<0.001; 95% CI=0.135–0.459).
DISCUSSION
This study advanced understanding of the psychological mechanisms that shaped health-protective intentions during a public health crisis. Perceived knowledge emerged as a key antecedent, significantly influencing both coping and threat appraisals. Individuals with greater knowledge were more likely to perceive a health threat as both serious and manageable, consistent with past findings in risk communication and protection motivation research [17,41]. This dual appraisal strengthened perceived control and increased motivation to adopt protective behaviors.
The results further clarified the distinct roles of coping and threat appraisals in shaping moral and social determinants of behavior. Coping appraisal significantly predicted moral obligation but not social approval. This pattern suggested that when individuals felt capable of effectively responding to a health threat, they internalized protective behaviors such as mask-wearing as a personal responsibility rather than a socially driven action. In contrast, threat appraisal significantly predicted both social approval and moral obligation, indicating that heightened threat perception activated both normative expectations and moral concern. These findings aligned with prior research demonstrating that perceived threat can heighten conformity to social norms and moral expectations [50]. Moral obligation emerged as the most influential predictor of mask-wearing intention, whereas social approval did not significantly affect intention. This finding may reflect two complementary explanations. First, in voluntary, post-mandate contexts, health-protective behaviors are more likely governed by internalized values than by perceived social pressure, thereby diminishing the predictive role of normative influence. Second, the non-significance of social approval may partly reflect the relatively narrow operationalization of subjective norms in this study. By conceptualizing subjective norms as social approval, emphasizing the prosocial dimensions of masking, the measure may not have fully captured broader normative pressures such as injunctive norms or social conformity. Similarly, attitude was operationalized as moral obligation, which, while appropriate for the voluntary behavior context examined here, did not encompass the full range of attitudinal dimensions posited by TRA, such as instrumental attitudes. Behavioral intention subsequently predicted actual mask-wearing behavior, supporting established theories linking intention to action [33]. Consequently, these results underscore the importance of integrating cognitive evaluations with moral processes when examining voluntary health-protective behavior.
This study extended PMT by formally incorporating TRA constructs, specifically moral obligation and social approval, into a unified framework for explaining voluntary health-protective behavior. Few studies have integrated these two theories in this manner, particularly in post-mandate contexts where behavior is driven by internal rather than external motivation. This integration advanced theoretical understanding by linking cognitive appraisal processes with normative and attitudinal pathways, offering a more comprehensive account of adaptive responses. Furthermore, the findings demonstrated that perceived knowledge shaped behavioral intentions indirectly through both coping and threat appraisals, highlighting the importance of examining mediating mechanisms in health-protective behavior models.
The results offered several actionable insights for public health communication. Campaigns should emphasize clear, accurate knowledge to strengthen coping efficacy and reinforce individuals’ moral responsibility to protect themselves and others. Messages that frame mask-wearing as an act of safeguarding the community may activate moral obligation more effectively than compliance-based appeals. Strengthening social norms through trusted community leaders, public health ambassadors, or influential figures may also enhance message credibility and collective engagement [8,36]. Such integrated messaging strategies may promote sustained preventive behaviors across diverse public health contexts.
Although the present study was conducted within a U.S. context, the findings may carry broader implications for public health practice in other countries, including South Korea. South Korea has demonstrated consistently high rates of voluntary mask adoption during and beyond the COVID-19 pandemic, a pattern that aligns with the central role of moral obligation identified in the present study. Cultural values that emphasize responsibility toward others and community well-being may further amplify the influence of internalized moral motivation on health-protective behavior. Future research should examine whether these findings generalize across cultural contexts, and comparative studies between the United States and South Korea may offer particularly valuable insights given their contrasting cultural orientations toward individual and collective health responsibility.
Conclusion
This study integrated PMT and TRA to explain how individuals form intentions and engage in voluntary health-protective behaviors. The findings highlighted the central influence of cognitive appraisals, particularly perceived knowledge and efficacy, alongside moral obligation in shaping protective intentions and actions. By demonstrating how cognitive, social, and moral determinants interact, the study provided a theoretically grounded and empirically supported account of the psychological mechanisms that drive preventive behavior.
The conceptual model developed here extends beyond the context of COVID-19. Its emphasis on perceived control, ethical responsibility, and internalized motivation offers a transferable framework for understanding a wide range of health-protective behaviors, including vaccination, respiratory hygiene, and chronic disease prevention. Integrating cognitive appraisal with moral and social motivations clarifies how individuals translate understanding into action. These insights can inform public health communication, behavior change strategies, and emergency preparedness planning.
Notes
AUTHOR CONTRIBUTIONS
Dr. Changhyun NAM had full access to all of the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis. All authors reviewed this manuscript and agreed to individual contributions.
Conceptualization: CN, HYY, and JL. Data curation: CN and HYY. Formal analysis: CN and HYY. Investigation: CN. Methodology: CN and HYY. Validation: CN and HYY. Visualization: CN and HYY. Writing–original draft: all authors. Writing–review & editing: all authors.
CONFLICTS OF INTEREST
No existing or potential conflict of interest relevant to this article was reported.
FUNDING
None.
DATA AVAILABILITY
The data supporting the findings of this study are not publicly available due to ethical and privacy restrictions involving human participants but are available upon reasonable request from the corresponding author.
ACKNOWLEDGMENTS
The author(s) would like to express gratitude to the Jim Moran College of Entrepreneurship, Health and Human Performance, and the School of Human Sciences for their support and encouragement throughout this endeavor.