

INTRODUCTION
Coronavirus Disease 2019 (COVID-19), caused by the SARS-CoV-2 virus, was first identified in Wuhan, Hubei Province, China, in November 2019 [1]. In response to the outbreak, the development of COVID-19 vaccines proceeded with unprecedented speed. Following Emergency Use Authorization (EUA), sequential vaccination campaigns were implemented worldwide to mitigate the impact of the pandemic.
The administration of COVID-19 vaccines has been shown to reduce the risk of infection and decrease the fatality rate of COVID-19 [2,3]. According to a June 2022 report from the Korea Disease Control and Prevention Agency, the effectiveness of the fourth dose of the COVID-19 vaccine compared to the third dose was 20.3% for preventing infection, 50.6% for preventing severe disease, and 53.3% for preventing death [4]. As of October 2022, the vaccination coverage rates in the Korean population were 87.9% for the first dose, 87.1% for the second dose, 65.6% for the third dose, and 14.7% for the fourth dose [5].
However, concerns about the safety of COVID-19 vaccines persist. A U.S. survey revealed that 31.6% of 991 participants would decline vaccination due to concerns about the vaccine itself and the need for more information [6]. Similarly, a 2021 survey in South Korea found that 49.4% of respondents who were unvaccinated cited perceived high risks associated with vaccination, rather than health issues, as the primary reason for their hesitancy [7].
Vaccination is essential for public health in the context of emerging infectious diseases. Despite its effectiveness in preventing such diseases, subjective perceptions about vaccines may result in delays or insufficient vaccination coverage. Previous studies have shown that subjective health status [8,9] and depression [10,11] can influence vaccination behavior for general or COVID-19 vaccines, but no research has directly analyzed the relationship between these factors. This study aims to evaluate the impact of COVID-19 vaccination on individuals by analyzing data from the Community Health Survey. It examines the relationship between demographic characteristics, depression, subjective health status, and COVID-19 vaccination.
METHODS
Study participants
Based on Article 2, Clause 2 of the Enforcement Rule of the Bioethics and Safety Act, this study does not fall under human subject research and is therefore exempt from review.
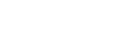
This study utilized raw data from the 2021 Community Health Survey, an annual statistical survey conducted by the Korea Disease Control and Prevention Agency. The survey assesses the health status of South Korean residents and informs evidence-based health policies. It targets adults aged 19 and older across various regions and housing types. Conducted from August 16 to October 31, 2021, the survey included 229,242 participants. For this study, five individuals who did not report their COVID-19 vaccination status and 25,788 individuals ineligible for vaccination were excluded from the analysis (Fig. 1).
The survey questionnaire was structured into household and individual sections, encompassing 18 domains and 163 questions. The household section addressed household type, basic livelihood support status, annual income, and changes in income and essential expenditures due to COVID-19. The individual section covered a range of topics including smoking, alcohol consumption, safety awareness, physical activity, dietary habits, obesity, weight management, oral health, mental health, vaccinations, screenings, chronic conditions (e.g., hypertension, diabetes), healthcare utilization, accidents, addictions, activity limitations, quality of life, social and physical environment, personal hygiene, educational and economic activities, and COVID-19-related issues.
Variables definitions
This study utilized demographic variables including age, sex, education level, household income, and health literacy. Age was categorized into two groups: 19–39 years and 40 years or older. Education level was classified into three categories: less than middle school, high school graduate, and some college or higher. Household income, measured as a monthly average, was divided into three groups: less than 3 million KRW, 3 million to less than 6 million KRW, and 6 million KRW or more. Health literacy was assessed based on responses to items concerning ‘understanding medical explanations from healthcare providers’ and ‘comprehension of information from sources such as newspapers, magazines, and the internet.’
The individual health status variables used in this study included subjective health status, depression, and morbidity (hypertension, diabetes). Subjective health status was reclassified from the survey items, with ‘very good,’ ‘good,’ and ‘fair’ being categorized as good subjective health status, and ‘poor’ and ‘very poor’ being categorized as poor subjective health status. For depression, the Patient Health Questionnaire-9 (PHQ-9), a self-reported survey consisting of nine items that correspond to the diagnostic criteria for major depressive disorder, was used from the survey items [12]. A score of 10 or higher, which indicates moderate depression, was defined as having depression, while a score of less than 10 was defined as not having depression.
Statistics analysis
In adherence to the guidelines for utilizing raw data from the 2021 Community Health Survey, the analysis employed a complex sample design with weighted data. Chi-square tests were conducted to assess differences in COVID-19 vaccination status based on demographic characteristics and individual health status variables.
To further explore the relationship between depression and vaccination status, the analysis excluded five non-respondents and 25,788 individuals who had not yet been scheduled for vaccination among the unvaccinated. The chi-square tests were then conducted to examine the association between vaccination status, depression, and subjective health status. Depression was categorized into two groups based on PHQ-9 scores: those with a score of 5 or higher and those with a score of 10 or higher.
To determine whether depression and subjective health status independently influence COVID-19 vaccination, multiple logistic regression analysis was performed, adjusting for age, sex, education level, household income, health literacy, and morbidity (hypertension and diabetes). IBM SPSS Statistics version 24.0 (IBM Corp.) was used for the analysis, and the statistical significance level was set at less than 0.05.
RESULTS
General characteristics of study participants
Table 1 summarizes the basic characteristics of the study participants. Higher vaccination rates were associated with older age, lower educational levels, higher income, better comprehension of medical explanations, lower depression levels, higher subjective health status, and the presence of hypertension or diabetes. Sex and the ability to understand written materials, such as newspapers and magazines, did not show a significant relationship with vaccination rates.
Comparison of COVID-19 vaccination according to depression and subjective health status
Table 2 compares COVID-19 vaccination rates by levels of depression and subjective health status. Groups with a PHQ-9 score of 5 or higher (88.5%), a PHQ-9 score of 10 or higher (84.4%), and those reporting Poor subjective health status (89.0%) exhibited significantly lower vaccination rates compared to their counterparts (P<0.001).
Association between depression, subjective health status, and non-vaccination
Table 3 presents the results of logistic regression analyses investigating the relationship between depression, subjective health status, and non-vaccination. Given that vaccination policy in South Korea prioritized older adults [13], a univariate analysis adjusted for age was performed. Additionally, a multivariate analysis was conducted, adjusting for age, education level, income, health literacy, and comorbidities (hypertension and diabetes).
In the age-adjusted analysis, all groups exhibited significantly higher odds ratios (ORs) for non-vaccination: PHQ-9 scores over 5 (OR=1.63; 95% confidence interval [CI], 1.56–1.71), PHQ-9 scores over 10 (OR=2.32; 95% CI, 2.12–2.54), and poor subjective health status (OR=2.73; 95% CI, 2.58–2.88). The multivariate analysis also revealed significantly higher ORs for non-vaccination in all groups: PHQ-9 scores over 5 (OR=1.52; 95% CI, 1.45–1.59), PHQ-9 scores over 10 (OR=2.00; 95% CI, 1.82–2.19), and poor subjective health status (OR=2.49; 95% CI, 2.35–2.64).
Impact of chronic diseases on subjective health status
This study classified depression and subjective health status as psychosocial factors and hypothesized that specific chronic diseases might influence subjective health status. For sensitivity analysis, participants were grouped into four categories: (1) good subjective health status without chronic diseases, (2) good subjective health status with chronic diseases, (3) poor subjective health status without chronic diseases, and (4) poor subjective health status with chronic diseases. Chronic diseases considered in the analysis were hypertension and diabetes, as identified in the 2021 Community Health Survey.
Table 4 presents the results showing that individuals with good subjective health status and chronic disease had the lowest OR for non-vaccination (OR=0.42; 95% CI, 0.39–0.45). Conversely, individuals with poor subjective health status, even without chronic disease, had the highest OR for non-vaccination (OR=1.89; 95% CI, 1.76–2.02). Those with both chronic diseases and poor subjective health status had a high OR (OR=1.13; 95% CI, 1.06–1.21). These findings indicate that subjective health status influences vaccination rates, regardless of the presence of chronic disease.
DISCUSSION
This study explored the relationship between depression, subjective health status, and COVID-19 vaccination. Using data from the 2021 Community Health Survey, we identified that higher vaccination rates were linked to older age, lower education levels, higher income, better understanding of medical explanations, lower depression levels, better subjective health status, and the presence of hypertension and diabetes. Logistic regression analysis revealed that higher levels of depression and poorer subjective health status were associated with lower vaccination rates.
Despite its rapid emergence and spread, COVID-19 has shown improved prevention efficacy through repeated vaccinations, akin to other novel infectious diseases [2,3]. The swift development and deployment of COVID-19 vaccines under EUA, coupled with limited initial clinical data, raised concerns about their safety. Extensive media coverage of adverse events associated with these vaccines under EUA has heightened public anxiety. A 2021 survey conducted by a South Korean broadcaster revealed that 41.8% of 1,093 respondents considered the COVID-19 vaccines to be “somewhat unsafe” or “not safe at all” [7]. Additionally, another South Korean study found that individuals exposed to media reports emphasizing vaccine side effects perceived a higher risk associated with COVID-19 vaccination and were consequently less likely to express intent to get vaccinated [14].
In this study, we found that poorer self-perceived health status was significantly associated with lower COVID-19 vaccination rates. This finding aligns with previous research indicating that individuals with poorer subjective health status are more likely to engage in health check-ups and receive influenza vaccinations [8,9]. Conversely, subjective health status is positively correlated with most health-promoting activities [8]. This trend suggests that individuals with worse subjective health status may suffer from chronic illnesses, leading to increased participation in “selective health-promoting activities” such as influenza vaccination and routine health screenings. It can be inferred that as disease prevalence rises, these individuals are more likely to frequent healthcare facilities and be exposed to health-related information, thereby increasing their “health-related sensitivity” [15,16].
Our study also indicates a relationship between depression and COVID-19 vaccination status. This finding is consistent with prior research demonstrating that mental health conditions impact vaccine willingness. A Japanese study reported that mental health issues such as depression, generalized anxiety, and low levels of fear regarding COVID-19 are associated with vaccine hesitancy or indecision [10]. Similarly, an American study found that individuals with depressive symptoms were more likely to believe misinformation about vaccines [11]. This suggests that individuals with depression may perceive fewer benefits from vaccination due to distorted information, potentially leading to lower vaccination rates.
Factors positively influencing vaccination uptake include self-efficacy and perceived benefits, which are among the most significant determinants [17]. This is consistent with previous research on both influenza vaccination intentions and COVID-19 vaccine uptake [18,19]. Self-efficacy is defined as an individual’s belief in their ability to successfully perform a task, including the completion of subsequent vaccine doses [18]. A well-established correlation exists between self-efficacy and depression [20]. The reduced self-efficacy often observed in individuals with depression may contribute to lower vaccination rates within this population.
From the perspective of perceived benefits and vaccination rates, it is reasonable to assert that an increase in perceived benefits of vaccination correlates with higher vaccination rates. A recent study involving American adults found that the risk of believing misinformation about the COVID-19 vaccine escalates with the severity of depressive symptoms [21]. This suggests that individuals with depression are more susceptible to accepting distorted information about the vaccine, which may adversely affect their perception of its benefits.
The limitations of this study are as follows. First, this study utilized data from the Community Health Survey which is cross-sectional in nature. It is unable to establish direct causal relationships or temporal sequences between self-perceived health status, depression, and vaccination status. Second, the assessment of depression and self-perceived health status was dichotomous, restricting the ability to perform more detailed quantitative analyses. Third, although adjustments were made for confounding variables within the Community Health Survey, factors not included in the dataset—such as prior adverse vaccine reactions, specific government policies at the time of vaccination, and the prevailing epidemic conditions—could not be accounted for. Fourth, this study considered hypertension and diabetes as chronic diseases related to subjective health status and depression but did not account for the potential influence of other chronic disease on prevalence and vaccination status.
Despite its limitations, this study demonstrates an association between vaccination rates and psychosocial factors concerning COVID-19 vaccination among the South Korean population. For future public health policies addressing emerging infectious diseases, it is crucial to consider various psychosocial factors. Ensuring the dissemination of accurate vaccine information and implementing strategies to enhance individuals’ self-efficacy and perceived benefits of vaccination can aid in the development of more effective prevention policies.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print



