

INTRODUCTION
According to the 2021 National Survey on Sports Participation in Korea, bodybuilding accounts for the highest proportion among sports activities of individuals in their 20s, comprising 30.8% [1]. Bodybuilding primarily involves resistance training, and the high participation rate among young adults indicates a considerable engagement in resistance exercises. People unfamiliar with resistance training because of a lack of regular physical activity may experience muscle damage due to sudden muscular contraction [2-4]. Such abrupt muscle damage can cause injuries or muscle soreness, restricting continuous participation in exercise [5]. Thus, effective recovery methods are necessary to alleviate muscle pain and damage.
Methods for muscle relaxation include foam rolling, massage, and stretching. Among them, foam rolling is the most commonly used tool for muscle relaxation because of its cost-effectiveness, convenience, and time efficiency [6-8]. Foam rolling helps reduce muscle stiffness by relaxing the adhered muscle fascia, thereby increasing joint flexibility and alleviating muscle fatigue and pain [9]. However, it has been observed that the muscle relaxation effects of foam rolling may be temporary, with limitations in sustaining long-term effects [10].
Recently, vibrating foam rollers, which integrate vibration with conventional foam rollers, are being utilized in practical applications. Among recovery methods for muscle fatigue, vibration stimulation inhibits sympathetic nervous system activities, allowing relatively prolonged muscle relaxation effects [11,12]. Combining vibration stimulation with foam rolling has helped sustain such effects [13], enhance mitochondrial biogenesis, and reduce inflammatory cytokines while activating the FAK pathway to promote muscle fascia decomposition [14]. This combination may further reduce muscle stiffness [14,15]. Thus, the synergistic contribution of the combined vibration and foam rolling stimulation may positively alleviate muscle damage and improve the joint range of motion (ROM) [11,12]. Accordingly, recent research has compared vibration foam rollers that integrate vibration functionality into traditional foam rollers [16]. Kasahara et al. [13] conducted a crossover study involving adult males and compared the effects of vibration foam rollers and regular foam rollers applied to the quadriceps femoris on muscle stiffness. They found that stiffness significantly decreased immediately after application of regular foam rollers; however, it returned to pre-intervention levels 20 and 30 minutes after application. Conversely, the application of vibration foam rollers significantly decreased stiffness not only immediately post-application but also 20 and 30 minutes post-application. Alonso-Calvete et al. [16] also suggested that vibration foam rollers demonstrate longer-lasting effects than regular foam rollers do. Typically, vibration foam rollers are used either before or after exercise. However, their indiscriminate use in practice persists because of unclear optimal timing for effective recovery from muscle and tissue damage and pain caused by resistance exercise. Thus, further research should determine the optimal timing of the application of vibration foam rollers in practical settings. Applying a vibration foam roller before resistance exercise may disrupt cross-bridges between actin and myosin filaments formed naturally when muscles are not contracted, thereby reducing tissue stiffness [17]. However, immediately after disrupting, cross-bridges gradually reattach; because of elastic recoil, the reattachment time can be shortened, potentially returning quickly to a stiff state [18]. Following resistance exercise, stimulation from a vibration foam roller can reduce the number of cross-bridges that increased due to elastic recoil, but subsequent reattachment may proceed slowly as elastic recoil does not occur thereafter [4]. This phenomenon suggests that it may effectively reduce stiffness after resistance exercise. Therefore, we hypothesized that applying a vibrating foam roller after resistance exercise may be more effective than that before resistance exercise. While conventional foam rollers have positively affected muscle recovery, they are limited by temporary efficacy. As such, further direct comparative studies should be performed on the recovery outcomes of the timing of the application of vibrating foam rollers, which can be used before or after resistance exercise in practical settings to complement these effects. Therefore, this study aimed to determine the optimal timing of the application of vibrating foam rollers, that is, before and after resistance exercise, by comparing the changes in serum creatinine kinase (CK) levels, ROM, and muscle stiffness.
METHODS
Participants
Twelve healthy adult males aged 19 years or older were recruited as participants. The selection criteria were as follows: (1) individuals who had not engaged in regular training over the past 6 months, (2) those without musculoskeletal issues, and (3) those without any significant medical conditions. The participants voluntarily expressed their intention to participate through recruitment notices and received information regarding protocols and precautions before the experiment. All participants signed their informed consent forms. They were randomly assigned to one of the following conditions in a single-group crossover design: pre-application of vibration foam roller (VF-PRE), post-application of vibration foam roller (VF-POST), or resistance exercise without vibration foam roller application (CON). For randomization, the protocol was conducted in three groups based on their sequential arrival at the laboratory. Their physical characteristics are presented in Table 1. The study was approved by the Institutional Review Board of the Korea University Institutional Review Board (IRB no. KUIRB-2023-0075-01).
Based on the research design, a sample of twelve participants was determined using G*Power software version 3.1 (https://gpower.software.informer.com/3.1). The effect size (η2=0.14) was set for analysis of variance (ANOVA): Repeated measures, within-between interaction, with a significance level of 0.05 and statistical power of 0.85.
Protocol
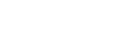
In the experimental design, the effects of applying a vibrating foam roller before and after resistance exercise on blood CK levels, muscle stiffness, and ROM were compared. Prior to baseline measurements, body composition, knee flexion ROM, and stiffness of the quadriceps femoris muscle were assessed, and a one-repetition maximum (1RM) test was performed. Stable pre-exercise blood samples for CK measurement were collected before each of the three exercise protocols.
Following the baseline measurements, all participants underwent the following exercise protocols in random order with a wash-out period of at least 5 days between protocols: VF-POST, VF-PRE, and CON. Post-measurements were conducted immediately after the exercise protocol and at 24 and 48 hours thereafter to determine the knee flexion ROM, muscle stiffness, and blood CK levels. Resistance exercise was performed at 80% of the 1RM, consisting of 6 repetitions with 1 minute intervals between sets, totaling 10 repetitions. The vibrating foam roller was applied to the rectus femoris at 2,700 rpm (approximately 45 Hz) for 60 seconds per leg by using a metronome set at 50 beats per minute (Fig. 1).
Body composition assessment
All study participants were instructed to wear light clothing during the experiments. Their height and weight were measured using a height–weight scale (BSM 340; Biospace), and body mass index (kg/m2) was assessed using a bioelectrical impedance analysis device (Inbody 570; Biospace).
One-repetition maximum test
A 1RM test was conducted to determine the weight for 80% of 1RM resistance exercise for the leg extension. The participants performed five preparatory exercises with weights of 5–10 kg. After the warm-up, they carried out 1–2 repetitions at 50%–60% of their estimated 1RM based on body weight. If the full ROM was achieved without difficulty, the weight was increased by 5 kg after a 2 minutes rest. If the full ROM was not achieved, the weight was decreased by 5 kg for the subsequent attempt. This process was repeated until the maximum weight that allowed full knee extension was determined as the 1RM.
Knee flexion range of motion
In the measurement of knee flexion ROM, the participants were instructed to lie on a prone position on a mat and flex their right knee joint maximally. A goniometer was used to measure the angle of knee flexion. Measurements were conducted by the same researcher under consistent environmental conditions throughout the experiment. Each knee flexion measurement was repeated twice, and the average value was recorded.
Muscle stiffness
The stiffness of the rectus femoris, a part of the quadriceps femoris group stimulated during leg extension exercises, was measured and assessed using a digital durometer (Shore C durometer; Generic). In this procedure, the distance from the anterior superior iliac spine to the upper border of the patella along the direction of muscle fibers was determined. Then, a point at the 2/3 distance was marked, and stiffness was measured with a durometer.
Creatinine kinase
All study participants were subjected to venipuncture to measure their CK levels. Prior to venipuncture, they were instructed to fast for at least 3 hours. Blood samples were collected via the antecubital vein. Approximately 2 mL of blood was drawn each time at four intervals (pre-, post-, 24 hr post-, and 48 hr post-exercise). A total of 12 blood samples were collected from each participant.
Statistical analysis
Data were statistically analyzed using Jamovi ver. 2.5.5 (The Jamovi Project 2024 [computer software]; retrieved from https://www.jamovi.org). All measurement variables were presented as means and standard deviations. Differences within groups and between time points were assessed via two-way repeated measures ANOVA, followed by Bonferroni post hoc tests. The statistical significance level was set at a=0.05.
RESULTS
Creatinine kinase
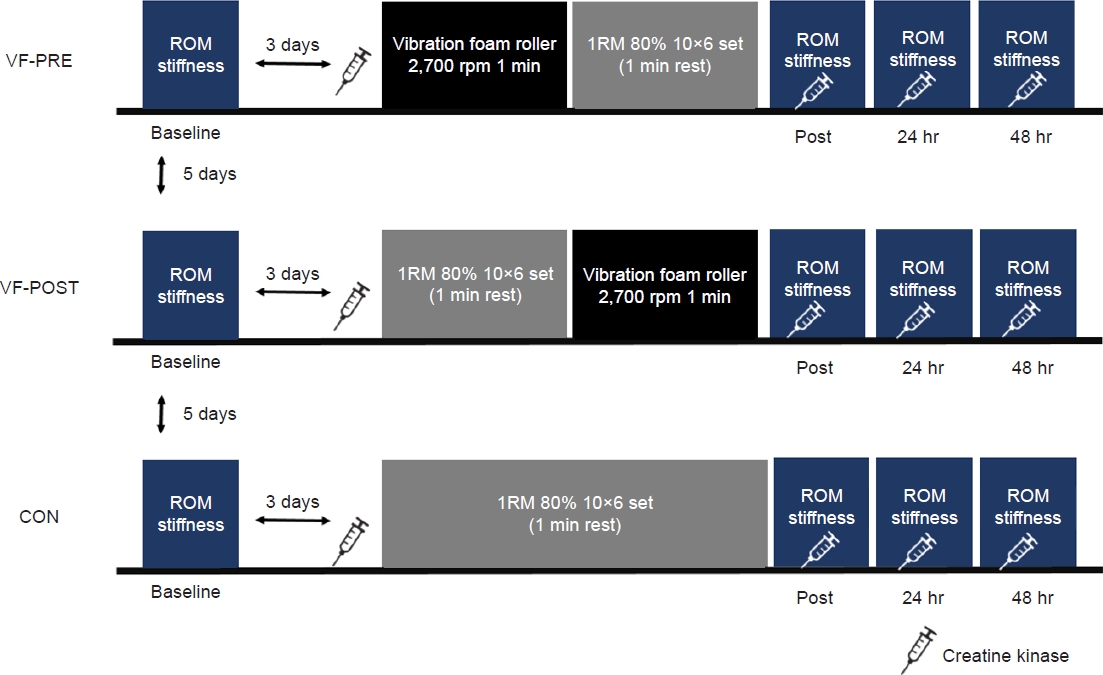
Changes in CK levels are depicted in Fig. 2. Two-way repeated measures ANOVA revealed that time points and groups had a significant interaction effect on the changes in the CK levels: F (6, 72)=14.7, P<0.001. Post hoc comparisons between groups at different time points indicated significant differences immediately post-exercise between CON and VF-PRE (P<0.001) and between CON and VF-POST (P<0.05). No significant differences were observed between VF-PRE and VF-POST (P=0.776). At 24 and 48 hours post-exercise, significant differences were found between CON and VF-POST (P<0.001) and between VF-PRE and VF-POST (P<0.05).
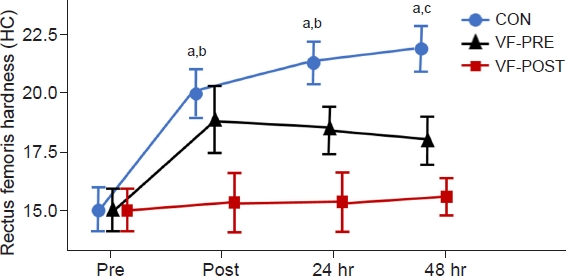
Stiffness of the rectus femoris muscle
The changes in the stiffness of the right rectus femoris muscle are presented in Fig. 3. Time points and groups showed a significant interaction effect on the changes in the stiffness of the rectus femoris (F=21.2, P<0.001). Post hoc comparisons between groups at different time points indicated that CON and VF-POST had significant differences immediately post-exercise (P<0.001). Conversely, CON and VF-PRE had no significant differences (P=0.6). Additionally, VF-PRE and VF-POST exhibited significant differences (P<0.05). At 24 hours post-exercise, significant differences were found between CON and VF-POST (P<0.001) and between VF-PRE and VF-POST (P<0.001). At 48 hours post-exercise, significant differences were observed between CON and VF-POST (P<0.001) and between CON and VF-PRE (P<0.001).
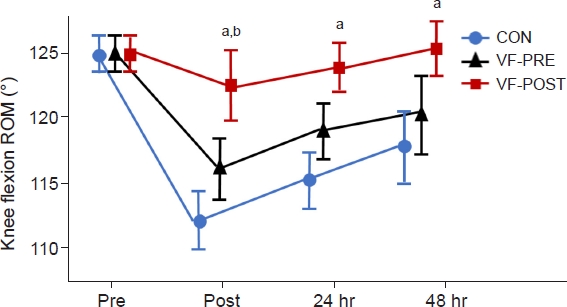
Knee flexion range of motion
The changes in the right knee flexion ROM are depicted in Fig. 4. Time points and groups exhibited a significant interaction effect on the knee flexion ROM (15.56, 35.19)=8.65, P<0.001. Post hoc comparisons between groups at different time points indicated significant differences between CON and VF-POST at all time points (P<0.05). Immediately post-exercise, significant differences were found between VF-PRE and VF-POST (P<0.05).
DISCUSSION
This study aimed to compare and analyze the effects of pre- and post-resistance exercise application of vibrating foam rollers on serum CK levels, muscle stiffness, and ROM in healthy adult males.
CK is commonly studied as an indicator of muscle damage; it typically increases when a muscle is injured. In this study, changes in CK levels showed that immediately post-exercise and at 24 and 48 hours post-exercise, CK levels were significantly lower in VF-POST than in CON; conversely, CK levels in VF-PRE were lower immediately post-exercise than those in CON, but they did not show significant differences at 24 and 48 hours post-exercise. Imtiyaz et al. [19] revealed that the CK levels of healthy females applying 50 Hz vibration stimulation for 5 minutes prior to endurance exercise were significantly lower 48 hours later than those of the control group without vibration stimulation. Kim et al. [20] applied vibration massage on the central part of the biceps brachii at 60 Hz for 5 minutes in a cross-over design, stimulation before resistance exercise, and stimulation after a washout period; then, they compared the changes in CK levels at 24, 48, and 72 hours later. They found that CK levels were significantly lower when vibration stimulation was applied after resistance exercise than when it was applied before resistance exercise. During eccentric contractions, muscle damage occurs due to sarcomere weakening, leading to the leakage of intracellular CK proteins into the bloodstream, resulting in increased plasma levels [21]. Vibrating foam rollers increase nitric oxide levels, promoting blood flow and enhancing endothelial function within blood vessels. They facilitate the removal of metabolic waste and activate muscle spindles via tonic vibration reflex, simultaneously stimulating muscle contraction and periarticular muscles. This activation increases heat generation, thereby reducing elastic stress in muscles and connective tissues, potentially lowering circulating CK levels. Consistent with previous findings, our results suggested that vibrating foam rollers might positively reduce CK levels. Additionally, the application of vibrating foam rollers after resistance exercise was likely more effective in reducing CK levels than that before resistance exercise.
Muscle stiffness can increase because of the accumulation of fatigue substances and muscle damage caused by eccentric contraction. Nevertheless, it can be reduced by self-myofascial release and vibration therapy.
In this study, we measured the muscle stiffness of the right rectus femoris. Immediately post-exercise and at 24 and 48 hours post-exercise, the stiffness in VF-POST was significantly lower than that in CON. At 48 hours post-exercise, stiffness significantly differed between the VF-PRE and CON groups, but no significant difference was observed immediately post-exercise and at 24 hours. Pournot et al. [4] reported that the shear modulus of the biceps brachii significantly decreased after localized vibration stimulation at 55 Hz on one arm subjected to a biceps curl at 70% 1RM in healthy adults. This result was consistent with the findings of the present study. Shear modulus is an indicator of muscle stiffness; it can increase because of the increased cross-bridge formation between myosin heads and actin following resistance exercise [22]. These cross-bridges can be partially disrupted by vibration stimulation [18], potentially reducing the increased stiffness observed after resistance exercise. However, applying vibration foam rollers before resistance exercise may not effectively reduce post-exercise stiffness because cross-bridges reattach shortly after disruption, and such reattachment increases with the subsequent contractile activity. Thus, applying vibration foam rollers after resistance exercise could be the most effective timing for reducing muscle stiffness.
The right knee flexion ROM was significantly lower in VF-POST than in CON immediately post-exercise, at 24 hours post-exercise, and at 48 hours post-exercise. Similarly, the right knee flexion ROM in VF-PRE was significantly lower immediately post-exercise than that in VF-POST. Resistance exercise-induced decreases in ROM may be attributed to inflammation caused by skeletal muscle damage, leading to fiber disruption and subsequent fibrous tissue adhesion [5]. Rahmani Nia et al. [23] induced muscle soreness in healthy adult males by performing leg extensions at 75% of 1RM with 3 minutes intervals until fatigue occurs to assess recovery effects. They observed that knee flexion ROM significantly decreased at 24 and 48 hours post-exercise compared with baseline measurements. Vibrating foam rollers can enhance tissue extensibility and muscle resilience by promoting blood flow and increasing muscle temperature [24,25]. Furthermore, stimulating Ruffini and Pacinian receptors, which inhibit sympathetic activities, can increase muscle relaxation [26]. In the present study, vibrating foam rollers possibly helped increase the ROM that decreased after resistance exercise. Lau and Nosaka [27] reported that the recovery of the elbow flexion ROM was significantly faster in the group that used Cybex to perform maximal voluntary eccentric exercises for the elbow joint followed by local vibration massage stimulation than in the control group. They observed that elbow flexion ROM, which typically decreases after eccentric exercise, recovered more rapidly with vibration stimulation. Conversely, Magoffin et al. [28] reported that applying whole-body vibration stimulation at 40 Hz for 60 seconds in five sets before maximal voluntary eccentric exercises with Biodex significantly decreased the knee flexion ROM at 24 and 48 hours post-exercise compared with baseline measurements.
Consistent with the present research, previous studies indicated that the post-eccentric contraction application of vibration foam rollers is effective in enhancing the ROM. The present results also showed that the extent of the decrease in ROM with VF-PRE was greater than that with VF-POST. This result suggested that the application of vibration foam rollers after resistance exercise positively influenced the reduction in muscle stiffness. Repetitive eccentric contractions increase the muscle stiffness after the resistance exercise, thereby decreasing joint flexibility. The stiffness of VF-POST was the lowest among the changes in muscle stiffness measured immediately post-exercise, at 24 post-exercise, and at 48 hours post-exercise. The changes in ROM also indicated that VF-POST effectively relaxed the stiffened muscles and tissues because of eccentric contractions, thereby positively influencing joint flexibility. Therefore, vibration foam rollers should be applied after resistance exercise to positively influence the recovery of knee flexion ROM.
This study confirmed that the application of vibrating foam rollers after resistance exercise is more effective than that before exercise in decreasing CK levels, improving joint flexibility, and reducing muscle stiffness. It also provides foundational data on the timing, frequency intensity, and duration of the use of vibrating foam rollers for practical application. However, this study has several limitations. Firstly, it only included adult males as participants. Secondly, we were unable to control for variations in dietary intake, sleep duration, and lifestyle habits among the study subjects. Future research should address the limitations and investigate how varying the frequency and duration of vibrating foam roller use affects muscle damage recovery.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print



