남성 대사증후군 유병률과 관련 요인 분석: 흡연 상태와 신체활동
Prevalence of Metabolic Syndrome and Related Factors Based on Smoking Status and Physical Activity in Korean Adult Men
Article information

Abstract
연구배경
흡연과 신체비활동은 각각 대사증후군(metabolic syndrome, MetS)의 유병률에 연관된 것으로 알려져 있다. 본 연구는 신체활동 수준과 흡연 상태에 따라 성인 남성에서 MetS의 유병률 및 관련 요인을 조사하기 위한 것이다.
방법
본 연구는 7기 국민건강영양조사(2016-2018)에 참여한 19-64세의 성인 남성 5,984명을 대상으로 분석을 실시하였다. 신체활동 수준은 저강도 활동(light physical activity, LPA), 중강도 활동(moderate physical activity) 및 고강도 활동(vigorous physical activity, VPA) 집단으로 각각 분류하였다. 흡연 상태에 따른 신체활동과 MetS의 관련성을 확인하기 위해 복합 표본 일반 선형모형과 로지스틱 회귀분석을 실시하였다.
결과
성인 남성에서 MetS 유병률은 27.8%로 나타났다. 흡연과 LPA의 증가는 MetS의 발병 위험을 증가시키는 것으로 밝혀졌다. MetS의 위험은 VPA와 quitter군에서 LPA와 흡연군에 비하여 64.7% 유의하게 감소하였다(교차비, 0.35; 95% 신뢰구간, 0.23-0.53).
결론
성인 남성에서 VPA가 MetS의 위험을 줄이는 효과적인 수단일 수 있으며, 흡연과 LPA는 MetS의 위험을 증가시킬 수 있다는 것을 시사한다.
Trans Abstract
Background
Cigarette smoking and physical inactivity are critical risk factors for the prevalence of metabolic syndrome (MetS). This study aimed to investigate the prevalence of MetS and its related factors in adult men based on their physical activity (PA) levels and smoking status.
Methods
In this cross-sectional analysis, 5,984 adult men aged 19-64 years were included based on the 7th Korean national health and nutrition examination survey (2016-2018). MetS was diagnosed based on the National Cholesterol Education Program Adult Treatment Panel III criteria, and PA was categorized as light PA (LPA), moderate, and vigorous PA (VPA). We used linear and logistic regression models to analyze the association between PA, MetS, and smoking status.
Results
The prevalence of MetS in adult men was 27.8%, with the risk of MetS increasing with smoking and LPA. The risk of MetS significantly reduced by 64.7% in the VPA and quitter groups compared to that in the LPA and smoking groups (odds ratio, 0.353; 95% confidence interval, 0.232-0.539; P=0.001).
Conclusions
Our study findings suggest that VPA may be an effective means of reducing the risk of MetS in adult men, while smoking and LPA may increase the risk of MetS.
INTRODUCTION
Metabolic syndrome (MetS) is a pathological state characterized by the clustering of multiple metabolic components, including abdominal obesity, hypertension, dyslipidemia, and impaired glucose tolerance, which increases the risk of cardiovascular diseases and type-2 diabetes mellitus, and are associated with all-cause mortality [1]. In Korea, the prevalence of MetS among adults increased from 21.6% in 2008 to 24.3% in 2017, and from 24.5% to 28.1% among adult men [2]. MetS is a consequence of the complex interactions between genetic and environmental factors. Unhealthy lifestyles such as smoking, alcohol consumption, and physical inactivity are associated with the incidence of MetS [3,4].
Physical activity (PA) has been shown to reduce the associated health risks of MetS even if individuals who exercise remain [5,6]. Increasing PA reduces weight and abdominal fat accumulation and improves insulin sensitivity [7]. An inverse dose-response relationship exists between PA and MetS, with high PA reducing the risk of MetS by 1.85-fold [8]. Vigorous PA (VPA) has been shown to prevents diseases associated with cardio-metabolism. In contrast, light PA (LPA) correlates with more chronic diseases [9], suggesting that increased PA intensity reduces MetS.
Smoking is a risk factor for MetS and affects lipid metabolism and insulin resistance [10,11]. The risk of MetS in current smokers is positively associated with the number of packs per year of smoking; quitters and current smokers with less than 10 packs of cigarettes have a significantly higher risk of MetS than those who have never smoked [12]. A meta-analysis showed that active smoking is associated with an increased risk of developing MetS (26%) compared to non-smoking [13].
Despite evidence that PA and smoking affect the risk of MetS in an individual, little is known about the comprehensive interaction of PA and smoking based on MetS and its components [14,15]. To the best of our knowledge, no studies have assessed the associations between MetS and specific combinations of smoking (i.e., never, quit, and smoker) and PA (i.e., LPA, moderate PA [MPA], and VPA). Additionally, studies examining the effect of PA on MetS prevention in smokers are limited and require further investigation.
We attempted to determine the relationships between smoking status, PA, and MetS in adult males using the 2016-2018 Korean National Health and Nutrition Examination Survey (KNHANES) data. The purpose of this study was two-fold: 1) to elucidate the relationship between PA and MetS and its components by considering the smoking status in men; and 2) to examine the risk of MetS according to the difference between smoking status and PA using the odds ratio (OR) of logistic regression.
METHODS
1. Data and participants
This study is a secondary data analysis utilizing information from the 7th KNHANES (2016-2018), conducted by the Korea Centers for Disease Control and Prevention [16]. The survey utilized a stratified multistage cluster probability sampling method to select a representative sample of civilians.
A flowchart depicting the subjects included in this study is presented in Figure 1. Of the initial 24,269 subjects who participated in the KNHANES, all females (n=13,198), males aged <19 and >64 years (n=4,648), and individuals with incomplete PA or smoking status (n=439) were excluded. Ultimately, 5,984 participants were included in the analysis. All participants in the KNHANES provided written informed consent, and the survey was approved by the Institutional Review Board of the Korea Centers for Disease Control and Prevention (approval no. 2018-01-03-PA). Since this study utilized a publicly accessible dataset, further ethical approval or informed consent was not required for the use of KNHANES data.
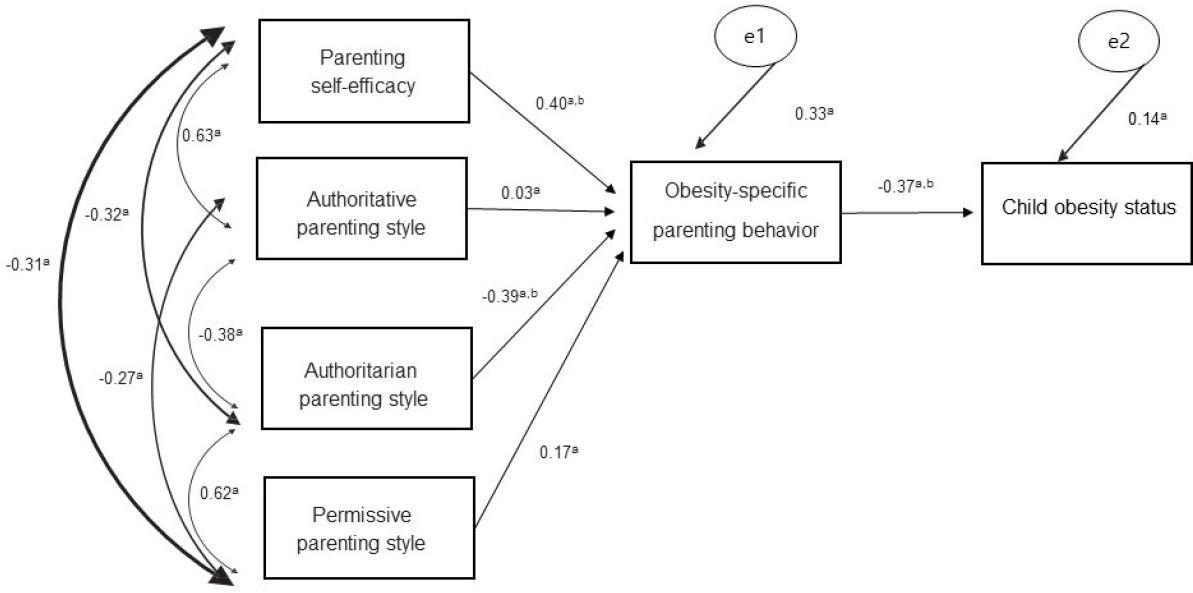
The path model in this study (n=61). The model’s fit showed a perfect fit to the data based on the results (χ2=1.22, df=4, RMR=0.016, RMSEA≤0.001, GFI=0.993, AGFI=0.965, NFI=0.988, CFI=1.00). The model’s fit showed a perfect fit to the data based on the results (χ2=1.22, df=4, RMR=0.016, RMSEA≤0.001, GFI=0.993, AGFI=0.965, NFI=0.988, CFI=1.00). df, degree of freedom; RMR, root mean square residual; RMSEA, root mean square error of approximation; GFI, goodness-of-fit index; AGFI, adjusted goodness-of-fit index; NFI, normed fit index; CFI, comparative fit index; AMOS, analysis of moment structures. aAll values indicate standardized coefficients using AMOS with maximum likelihood estimation obtained by the path analysis. bP<0.05.
2.Definition of the variables
1) Metabolic syndrome
This study used the National Cholesterol Education Program Adult Treatment Panel III clinical diagnostic criteria for MetS. For abdominal obesity, the Korean Society for the Study of Obesity's criteria for Korean adults were employed [17]. MetS was diagnosed if participants had three or more of the five symptoms: waist circumference ≥90 cm in men, triglyceride (TG) levels ≥150 mg/dL or under-treatment for increased triglyceride levels, fasting plasma glucose (FPG) levels ≥100 mg/dL or under-treatment for diabetes, high-density lipoprotein cholesterol (HDL-C) levels <40 mg/dL in men or under-treatment for reduced HDL-C, blood pressure ≥130/85 mmHg or use of antihypertensives.
2) Physical activity
PA was evaluated using the validated Korean version of the Global Physical Activity Questionnaire (GPAQ) [18,19]. The questionnaire consisted 16 questions about the frequency (days) and duration (minutes/hours) of moderate- and vigorous-intensity PA in three domains: work, leisure, and transportation. The GPAQ data were analyzed using the World Health Organization GPAQ analysis guidelines [20]. PA was calculated as metabolic equivalents (METs), which is the ratio of a person’s metabolic rate relative to the resting metabolic rate. One MET was equivalent to a caloric consumption of 1 kcal/kg/h. The MET for vigorous activity was 8.0 and that for moderate activity and transport (cycling and walking) was 4.0. The total PA MET (minute/week) was calculated using the following equation: place movement+moderate+vigorous MET (minute/week).
Participants were classified into one of three categories based on the official classification criteria: (i) vigorous: defined as a person reaching a vigorous-intensity activity on at least 3 days achieving a minimum of at least 1,500 MET min/week or ≥7 days of any of the combination of walking, moderate-or vigorous-intensity activities achieving a minimum of at least 3,000 MET min/week. (ii) Moderate: defined as a person not meeting the criteria above but meeting ≥3 days of vigorous-intensity activity of at least 20 minutes per day or ≥5 days of moderate-intensity activity or walking for at least 30 minutes per day or ≥5 days of any of the combination of walking, moderate- or vigorous-intensity activities achieving a minimum of at least 600 MET min/week. (iii) Light: defined as a person not meeting any of the above criteria.
3) Smoking status
Smoking status was self-reported, but information on the duration of cessation and the amount of tobacco consumed by current smokers was not provided in the KNHANES. Smoking exposure was categorized into three subgroups according to the Centers for Disease Control and Prevention (CDC) 1994 smoking criteria [21]: non-smokers (participants who had never actively smoked in their lifetime), quitters: (participants who had smoked more than five packs [100 cigarettes] but had quit before the survey), and current smokers (participants who smoked more than five packs [100 cigarettes] before the survey and continued to smoke at the time of the survey).
3. Anthropometric and biochemical parameters
The participants' weight and height were accurately measured to the nearest 0.1 kg and 0.1 cm, respectively, while they were wearing lightweight indoor clothing and had removed their shoes. Body mass index (BMI) was calculated as the ratio of mass (in kilograms) to the square of height (in meters). A standard mercury sphygmomanometer (Baumanometer; Baum, Copiague, NY, USA) was used by trained medical personnel to measure each participant's blood pressure in their right arm. Blood pressure readings were taken twice at a 5-minute interval, and the mean was calculated. Blood samples were collected from the anterior elbow vein after an overnight fast. The levels of FPG, TG, HDL-C, low-density lipoprotein cholesterol, and total cholesterol (TC) were analyzed using a Hitachi Automatic Analyzer 7600 (Hitachi, Tokyo, Japan).
4. Statistical analyses
The statistical analyses were conducted using KNHANES with weighted composite samples. Categorical variables were presented as unweighted numbers and weighted percentages, while continuous variables were expressed as means and standard errors. To determine differences in MetS components and prevalence based on smoking status and PA, a chi-square test was performed. Whenever a significant difference was detected, a Bonferroni-corrected post hoc test was conducted. A linear model that was adjusted for age was used to evaluate whether there were any significant differences between smoking status and PA regarding MetS and its components. Moreover, logistic regression was performed to examine the association between PA level and smoking status, taking into account covariates such as age and BMI. The results of logistic regression were presented as OR with 95% confidence intervals (CI). All hypotheses were two-tailed and a P-value of less than 0.05 was considered statistically significant. The analyses were performed using the SPSS version 26.0 (IBM Corp., Armonk, NY, USA).
RESULTS
Table 1 presents the baseline characteristics of the study participants according to smoking status. Among the 5,984 male participants, 1,663 (29.7%) were never smokers, 1,892 (29.8%) were quit smokers, and 2,429 (40.5%) were current smokers, based on the CDC's smoking criteria. The quitters were taller, heavier, had a larger waist circumference, and had higher BMI and HDL-C levels than the other two groups (P<0.05). Individuals who had never smoked had lower TC and FPG levels than the other two groups. Blood pressure and low-density lipoprotein cholesterol (LDL-C) levels did not differ significantly among the three groups. MetS was more prevalent among smokers and quitters than among non-smokers (P=0.001), and a lower proportion of smokers performed MPA and VPA than quitters and non-smokers (P=0.001).

Baseline characteristics of subjects according to smoking status
Table 2 presents the PA level and health-related indicators in non-smokers. Significant differences were observed in the TG, HDL-C, and LDL-C levels (P<0.05). Post-hoc analysis showed that the never smoking vigorous PA group (NVG) had a lower TG level than the never smoking light PA group (NLG) (P=0.037). The NVG had a higher HDL-C level than the NLG (P=0.001) and never smoking moderate PA group (NMG) (P=0.003). The NLG had a higher LDL-C level than the NMG (P=0.001). No significant differences were found in the other indicators among the groups (P>0.05).

Differences in health-related variables based on PA levels of never smokers
Table 3 presents the PA and health-related indicators in quitters. Significant differences were observed in the FPG, TG, and HDL-C groups (P<0.05). Post-hoc analysis showed that the quit smoking light PA group (QLG) had a higher FPG levels and lower HDL-C levels than the quit smoking moderate PA group (QMG) and quit smoking vigorous PA group (QVG) (P<0.05, respectively). TG levels in the QVG was lower than those in the QMG (P=0.013) and QLG (P=0.002).

Differences in health-related variables based on PA levels of quitters
Table 4 presents the PA and health-related indicators in smokers. The results indicate significant difference in BMI, HDL-C, and LDL-C levels (P<0.05). Further post-hoc analysis shows that the smoking vigorous PA group (SVG) has a lower BMI compared to the smoking light PA group (SLG) (P=0.006) and smoking moderate PA group (SMG) (P=0.006). Additionally, SMG has higher HDL-C levels than the SLG (P=0.001) and SVG (P=0.039), whereas SVG has lower LDL-C levels compared to SLG (P=0.019) and SMG (P=0.028).

Differences in health-related variables based on PA levels of smokers
Table 5 reports the multifactorial analysis of the effects of smoking status and PA on MetS and its components. The analysis was adjusted for multiple risk factors, and the findings suggest that smokers have a 67.8% increased risk of MetS compared to the non-smokers (OR, 1.678; 95% CI, 1.386-2.030; P<0.001), with a significantly higher risk of hypertriglyceridemia, low HDL-C levels, and increased glucose metabolism. On the other hand, quitters have a 23.3% reduced risk of low HDL-C levels (OR, 0.767; 95% CI, 0.641-0.917) compared to non-smokers. Moreover, performing LPA increases the risk of MetS by 54.8% (OR, 1.548; 95% CI, 1.188-2.017; P=0.001) and is associated with a higher risk of developing abdominal obesity and low HDL-C levels.

Multi-factorial analysis of smoking status or PA effects on metabolic syndrome and its components
Table 6 displays the logistic regression analysis of PA level and smoking status on MetS. The results show a significant interaction between smoking status and PA. Specifically, VPA in non-smokers reduces the risk of MetS by 59.9% compared to LPA smokers (OR, 0.401, 95% CI, 0.256-0.627; P<0.001). Furthermore, the risk of MetS decreases in an exercise intensity-dependent manner in smokers, quitters, and non-smokers.

Logistic regression of PA level and smoking status on MetS
DISCUSSION
This study aimed to investigate the relationship between PA levels and MetS based on smoking status. The results revealed several significant differences in PA levels and MetS and its components according to the smoking status. Smoking was found to increase the risk of MetS and its components, particularly in relation to abnormalities in TG, HDL-C, and FPG levels. Increasing PA intensity, on the other hand, was associated with a decreased risk of low HDL-C levels. Additionally, both smoking and PA showed a dose-dependent effect on risk of MetS. The adjusted OR for MetS risk showed a decrease throughout in an exercise intensity-dependent manner. However, the MetS risk in smokers only reduced with VPA, not with LPA or MPA.
Smoking is known to stimulates sympathetic activity, which results in the production of insulin-blocking hormones such as cortisol, catecholamines, and growth hormones. This, in turn, promotes lipolysis and increases plasma-free fatty acids, ultimately leading to the development of MetS. Previous studies have shown a significant association between smoking and low HDL-C levels, high TG levels, and diabetes [10,11]. Our study also found that smoking increased the risk of low HDL-C levels, high TG and FPG levels, and MetS in males (P=0.001), consistent with prior research [15]. We further discovered that smoking led to a reduction in weight and waist circumference, which was due to a decrease in lean body mass rather than fat loss, and may not be entirely distinguishable by BMI [11].
The beneficial effect of PA on cardiometabolic risk has been demonstrated by both cross-sectional cohort studies and structured exercise interventions. Our study found a significant, dose-dependent association between PA and MetS, as well as an exercise intensity-dependent association with high levels of HDL-C (P=0.001; Table 5). These findings are consistent with prior research demonstrating that PA enhances the activity of lipoprotein lipase, improves lipoprotein lipids, reduces TG levels, increases HDL-C and plasma adiponectin levels, and inhibits platelet aggregation and inflammation [22,23].
Moreover, our study revealed that quitters who engaged in MPA or VPA had lower FPG levels and a lower risk of MetS compared to quitters who engaged in LPA. This finding is in line with earlier research, which showed that replacing LPA and MPA with equal amounts of VPA was linked to a decreased risk of non-communicable diseases [14]. In particular, VPA was found to be more effective than LPA in reducing the risk of MetS [22]. Therefore, we recommend as a preventative measure against the development of MetS and its associated complications.
Our study results are consistent with previous prospective studies that have shown individuals may experience significant weight gain after quitting smoking [24]. Quitting smoking is associated with more weight gain than non-smokers, which may be due to reduced energy expenditure and increased appetite. While weight gain may diminish the health benefits of quitting smoking by increasing the risk of cardiometabolic diseases, the evidence is inconclusive [25]. In addition, our study found that the proportion of non-smokers engaging in moderate-to-vigorous intensity PA is much higher than that of smokers and quitters. PA levels generally increase after smoking cessation, which is consistent with previous research [26]. A previous review has assessed the relationship between exercise, PA, and smoking and concluded that smoking and PA were inversely associated, although the relationship is weak and unstable, the results of most of the cross-sectional surveys are consistent [27].
Our study also revealed an interaction between smoking and PA on the development of MetS. Light-to-moderate intensity PA reduced the risk of MetS in both non-smokers and quitters (Table 6). Notably, quitters who performed VPA had a significantly lower risk of MetS (OR, 0.353, 95% CI, 0.232-0.539) by 64.7% compared with those who engaged LPA. Furthermore, only VPA was protective against MetS in smokers (OR, 0.549; 95% CI, 0.354-0.850). Previous research has shown that PA may not significant protective effect against MetS development in smokers, which may be related to smoking intensity [28].
Our study also found that PA was not sufficient to compensate for the negative impact of heavy smoking. PA can reduce the risk of MetS in individuals without major cardiovascular risk factors, but its effect is not sufficient for those with high-risk factors [29]. Therefore, PA may prevent MetS in populations with low-risk factors. Therefore, smoking cessation is necessary to prevent the development of MetS, rather than promoting exercise alone in current smokers.
This study had several limitations that should be acknowledged. Firstly, the smoking status and PA levels were based on self-reported data, and we did not consider exposure to cigarette smoke in non-smokers. Although passive smoking is known to affect the risk for MetS, exercise capacity and cardiorespiratory function are not influenced by smoking status [30]. However, we did not collect information on the number of cigarettes smoked or the duration of quitting among current smokers, which can affect the risk for MetS. Moreover, reported that VPA does not have any protective effect in individuals who smoke ≥20 cigarettes/day [15]. Secondly, we did not consider other potential confounding variables, such as alcohol consumption and dietary habits, which may affect our findings. However, we included age and BMI, which are known risk factors for MetS. Finally, the cross-sectional design of our study precludes us from drawing causal inferences. Therefore, caution is warranted in interpreting our findings. Despite these limitations, our study provides valuable evidence on the association between smoking status, PA, and MetS in Korean adult males.
The adjusted OR for MetS risk decreased in an exercise intensity-dependent manner across all smoking groups. Specifically, only VPA was found to effectively reduce the risk of MetS in smokers. Therefore, it is recommended that individuals receive early and effective smoking cessation intervention. In the future, longitudinal cohort studies using objective measures such as pedometers and accelerometers should be conducted to confirm the causal relationships between the intensity and duration of smoking and PA in reducing the risk of MetS.