Attitudes, Perception and Preventive Behaviors for Health and Safety among College Students
Article information
Abstract
Background
The purpose of this study was to analyze the correlation between risk perception and attitudes and preventive behaviors among college students with poor health and safety consciousness.
Methods
A survey was conducted in students at three universities in the metropolitan area from May 11 to 18, 2018. Four kinds of instruments were used for this study, questionnaires about attitudes, perception, prevention education and preventive behaviors.
Results
The safety-related attitude depended on age: those aged <21 years had the best attitude. Education experience significantly affected perception. Preventive behaviors were more strongly and positively correlated with attitudes than with perception. The factor most significantly affecting preventive behaviors were attitudes to preventive health.
Conclusions
To allow the students to change their awareness and behaviors related to sickness and accidents, first it is necessary to give education on a continuous basis so that they can obtain perception to cope with sickness and accidents; second, it is necessary to develop behavioral guidelines related to accidents in each area so that they can practice and make it a habit through attitudinal changes.
Introduction
Korea Centers for Disease Control and Prevention requested to improve personal hygiene by washing hands properly to prevent a number of infectious diseases such as typhoid, Middle East respiratory syndrome (MERS) viral eye infection, and etc. Washing hands is the most basic step we can take to prevent infectious disease and 50–70 percentages of waterborne diseases can be prevented through simply washing hands. Though most Korean citizens are aware of important of hand hygiene, it's not being actively put into behavior.1) Fine dust, which has recently become a social issue publicized concerns about air pollution because it was found to be a potentially serious threat to human health. In contemporary society, the factors for environmental danger, such as fine dust, appear on a constant basis. Although environmental pollution significantly affects the quality of our life, causing serious environmental problems, such as yellow dust and fine dust, both environmental education and preventive support are rarely provided.2)
According to the Seoul online panel survey on safety consciousness, 56.7% indicated very weak safety consciousness and 39.5% weak safety consciousness, while approximately 96% of the respondents indicated that the South Korean society had weak consciousness.3) The statistical yearbook of the Ministry of Public Safety and Security reported that 23,525 (52.9%) out of 44,435 fire accidents in 2015 were due to carelessness.4)
Although many people worry about safety and health, the statistics of safety and health reveals a gap between ‘perceiving’ and ‘behavior’. 64.0% had never participated personally in education or training to prevent and cope with sickness or accidents while 98.7% suggested the need for such education and training. Those in their twenties were from 5.7 to 10.5% more likely to make such answers.5) The role of communication campaigns that lead to changes in cognition, attitudes, and behaviors in order to perform health activity is becoming more important.
An observational survey done identified that 73 percentages of public bathroom users wash their hands and only 33 percentages of them use soap when washing hands.1) As few as three out of 10 persons wore a mask when a “high” risk of fine dust was predicted; in particular, only 19% of those aged 19–29 years wore a mask.6) The preparatory exercise relieves the tense body and prevents the rapid increase of the blood pressure due to the rapid increase of blood flow. The rate of regular physical activity among Koreans aged 15 and over is very low at 32.1%.7) However, the study on the pre-exercise rate before physical activity is insufficient.
This study aimed to identify the factors affecting the perception of danger and activity to address them among people in their twenties. According to the four stages of changes in behavioral science, behavioral changes need to involve changes in ‘perception’ and ‘attitude’ which may lead to group or organizational performance.8)
Preventive behavior refers to a person or a group's beliefs and actions regarding their health and well-being.9) We need to identify factors that affect practicality in order to promote preventive behavior. The current study targeted a population of college students to specifically examine attitudes, and risk perception in relation to behavior, and their impact on activity.
Methods
1. Participants
The purpose of this study was to determine attitude and perception among college students coping poorly with accidents and identify the factors affecting their behaviors and practice. Students from three universities in the metropolitan area were extracted using convenience sampling. Data collection was performed from May 11 to 18, 2018. A total of 400 questionnaires were distributed; of these, 364 copies were returned.
2. Survey contents
The socio-demographic variables included gender, grade and age.
1) Attitudes
Attitudes towards health and safety are defined as following preventive health care measures and protecting oneself from danger. Public Safety Consciousness Index (PSCI) is to measure individuals' safety capability, behaviors, attitudes, habits, and knowledge in order to help prevent accidents and to minimize artificial disasters through safe actions in daily life, as well as in case of disasters and emergencies.10) The attitude of the study object took reference from this PSCI and the survey is sorted by health and safety related attitude. Attitudes towards health and safety were assessed in the following way: first, the respondents' attitudes levels were assessed on a four-point Likert scale, ranging from ‘very poor’ to ‘very good’.
Health-related attitude is evaluated with attitude to preventive health, such as checking ingredients and effects when taking medications, doing warm-up exercises prior to physical activities, checking expiration dates of food products, and attitude to environmental pollution, including checking air quality, wearing a mask when there is a fine dust warning. The health-related attitude of Cronbach's alpha is 0.680.
Safety-related attitude is evaluated with attitude to electrical safety such as precautions for using electrical equipment, how to use a plug, and attitude to traffic safety as seatbelt use, following safety signs, and attitude to fire safety, such as acknowledging how to use fire extinguishers and fire alarm evacuation. The safety-related attitude of Cronbach's alpha is 0.813.
2) Perception
Perception is defined as the concept of knowledge acquired through media, experience, and education (risk perception from the following). The risk perception to cope with accidents was determined, taking into account the instructions for action made by the Ministry of Public Safety and Security.11) The study identified knowledge of health and safety such as infection prevention measure, drug dosage, checking expiration dates, coping with fine dust pollution, precautions for gas and fire use, how to handle car accidents, preventing electrical accidents. Perception was classified as ‘knowing’ and ‘not knowing’.
3) Prevention education
Prevention education aims to provide knowledge necessary to lead a safe and healthy life and change attitudes or behaviors in a desirable direction and focuses on the efforts to cultivate ability to keep one or others from accidents or damages.12) To determine education status, the experience of getting the education before college entrance (learning experience; before admission), the experience of getting the education after college entrance (learning experience; after admission), effect of prevention education, understanding of prevention regulation as well as will to participate in the education, were examined. The learning experience was evaluated as ‘ever’ and ‘never’. The effect of prevention education and will to participate in education were evaluated as ‘yes’ and ‘no’. The understanding of prevention regulation was assessed on a four-point Likert scale, ranging from ‘very poor’ to ‘very good’.
4) Preventive behaviors
Self-evaluation about health and safety-related preventive behaviors were performed using a 10-point semantic scale to determine the level of maintaining safety and preventing accidents.
3. Statistical analysis
The collected data were analyzed using SPSS/WIN 23.0 program (IBM, Armonk, NY, USA), with significance probability set at 0.05. To test the hypotheses, the following statistical analyses were carried out: first, frequency analysis was performed to determine the respondents' general characteristics and cues to action; second, mean analysis and Fisher's exact test were performed to determine the differences in principal variables by such general characteristics and cues to action as gender, age, understanding of prevention regulation and effect of preventive education; third, correlation analysis was performed to determine correlation among principal variables; fourth, logistic and multiple regression analyses were performed to identify the factors affecting behavioral changes.
Results
1. Study participants
The respondents' general characteristics are as presented in Table 1. One hundred sixty-seven respondents were male and 197 were female. One hundred three respondents were freshmen, 72 sophomores, 97 juniors, and 92 seniors. One hundred thirty-five respondents were aged ≤21 years, 101 were aged 22–23 years, and 127 were aged ≥24 years. Fifty-seven respondents had never received preventive education and 307 had received it. One hundred fifty-seven respondents were not inclined to participate in education while 207 had affirmative inclination (Table 1).

General characteristics of study participants
2. Demographic variables
1) Attitudes
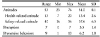
There were statistically significant differences in healthrelated attitude by gender: the mean score was 13.46 for 167 male, 13.36 for 197 female. There were statistically significant differences in safety-related attitude by age: the mean score was 38.68 for the respondents aged ≤21 years, 36.41 for those aged 22–23 years, and 37.43 for those aged ≥24 years (Table 2).

Attitude and perception according to general characteristics
2) Perception
As for the differences in perception by grade, the mean score was 2.92 for 103 freshmen, 3.60 for 72 sophomores, 3.44 for 97 juniors, and 3.51 for 92 seniors. The post-hoc test showed that sophomores and seniors scored higher on average than freshmen. As for the differences in perception by age, the mean score was 3.01 for the respondents aged ≤21 years, 3.59 for those aged 22–23 years, and 3.50 for those aged ≥24 (Table 2).
3. Prevention education
We considered the high and low levels of health and safety related attitudes in connection with the understanding of prevention regulation. Respondents with high level of health related attitude (152, 88.4%; row) had a higher understanding of prevention regulation (P=0.001). There were differences in levels of health related attitude (P=0.021) and safety related attitude (P<0.001) regarding the effect of prevention education. There were also differences in high and low levels on perception in experience of prevention education (P=0.007). Respondents with no education experience (41, 71.9%) had lower levels of perception than the ones with education experience (Table 3).

Attitude and perception according to preventive education
4. Correlation between attitudes, perception and preventive behaviors
The descriptive statistics for attitude, cognition, and preventive behaviors were calculated. For the attitudes, the minimum value is 23, the maximum value is 76, with an average of 51.0 and a standard deviation of 8.1. For perception, the minimum value is 0, the maximum value is 7, and the average 3.3 standard deviation is 1.4. For preventive behavior, the minimum was 1, the maximum was 10, the mean was 6.2, and the standard deviation was 1.8 (Table 4).
Descriptive statistics of attitudes, perception and preventive behaviors
Pearson's correlation analysis was carried out to determine the correlation among principal variables. Significant positive correlation was found between attitudes and preventive behaviors and between perception and preventive behaviors. No statistically significant correlation was found between attitude and perception (Table 5).

Correlation between attitudes, perception and preventive behaviors
5. Factors affecting to preventive action
The logistic regression analysis found that gender, understanding of prevention regulation, the experience of receiving education, and attitudes significantly affected preventive behaviors. The males showed 1.9 times higher levels of preventive behaviors than the females at the 5% significance level. The respondents with high levels of understanding of prevention regulation showed about 2.2 times higher levels of preventive behaviors than with low levels of understanding of prevention regulation. The respondents having received education showed about 2.8 times higher levels of preventive behaviors whereas the respondents with high levels of attitude showed about 3.1 times higher levels of preventive behaviors than those with low levels of attitude (Table 6).

Factors affecting to preventive behaviors using logistic regression
Multiple regression analysis was performed to determine the effects of perception, understanding of prevention regulation and attitude related to such independent variables as preventive health, environmental pollution, electrical safety, traffic safety and fire safety on the dependent variable, preventive behaviors. To perform the regression analysis, auto-correlation of the dependent variable and multicollinearity among the independent variables were determined. The Durbin-Watson index was used to determine the auto-correlation of the dependent variable. The dependent variable was independent without auto-correlation because Durbin-Watson was 1.890. VIF was used to determine multicollinearity among the independent variables. There was no multicollinearity because VIF among the independent variables was <10: 1.053–1.410. The multiple regression analysis showed that attitude to preventive health (B=0.238) and electrical safety (B=0.185) significantly affected the dependent variable and preventive behaviors. The respondents with better risk perception and attitude were more likely to do preventive behaviors, which accounted for 21.3% of the dependent variable. Of the independent variables, attitude to preventive health (β=0.227) more strongly affected preventive behaviors (Table 7).

Factors affecting to preventive behaviors using multiple regression
Discussion
This study aimed, first, to determine the level of perception about health and risk among college students in relation to the large scale and increase of accidents due to no definite measures, such as preventive education and training, and to suggest the need to give education on a continuous basis; second, to determine if behavior depended on the perceived risk. Ultimately, it intended to find a way to help those with poor changes in attitude and knowledge.
Through several researches, we discovered a link between knowledge of disease, disease awareness, and health improvement practice among various other factors.1314) This study aimed to determine the need to give education on a continuous basis and the effects of attitude and perception on preventive behaviors for college students with poor health and safety consciousness.
First, safety-related attitude and perception differed by age (P<0.05). The respondents aged ≤21 (38.68) showed higher levels of attitude than those aged 22–23 years (36.41). As for the differences in preventive behaviors by age, while the literature review14) showed that older individuals had higher index (e.g., the index was higher for ≥30 than for <30). The older nurse practitioners showed a higher level of hand-washing performance. Nurse practitioners with ≥5 years of career showed higher levels of hand-washing performance than those with <1 year of career. Presently, safety-related prevention education is regularly/mandatory from kindergarten through high school.15) Through these regular safety-related training, respondents are properly habituated to a safe attitude. Therefore, it was found that the attitude average was high at the age of 20 years or younger. These results suggest that it is more important to continue education and habituation at educational institutions such as age 21 or university where independent life begins.
Second, attitudes were more strongly and positively correlated with behavior. Attitudes made no statistically significant changes in perception (r=0.043, P>0.05). In contrast, perception and attitudes were significantly correlated statistically with preventive behaviors: those with better attitudes were actually more sensitive to health and safety and were highly likely to do preventive behaviors. As for the correlations between health belief in hand-washing and hand-washing practice, perceived susceptibility was positively correlated with hand-washing performance.16) Perceived health risk (β=0.135) had significant positive influences on health-related Internet use.17)
Third, education experience significantly affected perception. Respondents with low level of perception (41, 71.9%) had no education experience (P=0.007). Before university entrance, 307 respondents (84.3%) had received prevention education and 57 (15.7%) had never received it. In contrast, after university entrance, 119 respondents (32.7%) had received prevention education and 245 (67.3%) had never received it. This result demonstrates that while the elementary and secondary curriculums contain prevention education, universities fail to provide prevention education on a continuous basis. It is necessary to give preventive education for health and safety to the group aged ≥20 years, including college students.
Fourth, understanding of prevention regulation and education experience significantly affected preventive behaviors. After the safety education based on experiential learning, the experimental group was significantly better statistically at practice than the control group.18) This agreed with the finding of this study that preventive education led to better practice. The previous research that compared the safety index between before and after education reported an increase in the mean percentile score following education.19) In contrast, no significant change in the mean was found for perception and attitude by the experience of receiving education after college entrance. Study participants having received education before college entrance are 2.8 times more likely to do preventive behaviors than those having received no education. However, there was a statistical result that the experience of receiving education after college entrance had no effect on preventive behaviors. This result demonstrates that college students make few efforts to raise the safety index than elementary and secondary school students. This paper regarding education mostly reviews improvement in safety capability by other adults to prevent accidents in early childhood and adolescence,20) and the research focusing on college students report that they have poor consciousness and practice21) in campus life. Now it is necessary to discuss the need for preventive education for those in their twenties and the quality of the education.
Fifth, attitude to preventive health most significantly affects preventive behaviors. Attitude to preventive health more significantly affected preventive behaviors than attitude to environmental pollution. Study participants with good attitude were about 3.1 times more likely to do preventive behaviors than those with poor attitude. This result suggests the need for methods to promote the attitude to health. Although people who are sensitive to health and safety observe prevention regulations relatively well in daily life, observation of prevention regulations may not correspond to perception. The level of perception about coping with sickness and accidents has no positive association with behaviors unless one makes personal efforts to obtain it or unless obligatory education is given. prevention.com recommends to ‘wash hands properly’ and ‘get regular sun exposure’ especially in between seasons to prevent catching a cold. Guidelines on putting prevention into practice are in place to support preventive health activities. Guidelines such as preventive health activities need to be utilized in the field of safety.
It is necessary to make it a habit to have perception, functions, and attitudes through preventive education and have safe living attitude basically with the objective of creating a healthy social environment safe. For preventive education, therefore, it is necessary to maintain safe conditions and functional education for healthy and safe behaviors in living, and education related to attitudes of cultivating a habit to predict and prevent risk factors. Preventive education can be more effective when it is given by stages in a long term than in a short term, and such education can be most effective.
We were able to identify a significant relationship between disease awareness (perception) and attitude towards disease, aside from other factors that have impact on health improvement practice, in fields related to health and safety.
Notes
This study was supported by the Ministry of Science, ICT & Future Planning (NRF-2017R1A2B4006545).